Chapter 47 Tubal Disease
ETIOLOGY AND CLASSIFICATION
Tubal disease accounts for 25% to 35% of female infertility. The most common cause of tubal damage is pelvic inflammatory disease (PID) (Fig. 47-1A; Table 47-1). Furthermore, the incidence of subsequent tubal occlusion is proportional to the number of PID episodes.1 Other causes of tubal damage are ectopic pregnancy and iatrogenic tubal sterilization. A detailed discussion of the infectious causes of infertility is given in Chapter 33. In a smaller scale, in utero exposure to diethylstilbestrol (DES) has been implicated to cause fallopian tube abnormalities, such as foreshortened, sacculated, or convoluted tube.2
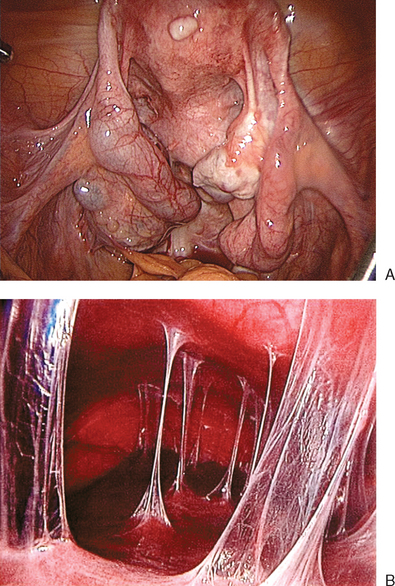
Table 47-1 Etiology of Tubal Disease
| Causes | Frequency |
|---|---|
| Pelvic inflammatory disease | 50% |
| Previous pelvic surgery | 27% |
| Iatrogenic posttubal sterilization | 1–3% |
| Endometriosis | 7–14% |
| Congenital anomalies | Rare |
EVALUATION OF TUBAL DISEASE
Hysterosalpingography
HSG is a contrast study of the fallopian tubes and the uterine cavity. It is widely used because it is simple, cost-effective, and associated with minimal side effects. Distal tubal blockage is usually associated with a hydrosalpinx. A potential limitation of HSG is tubal spasm, which can give a false impression of proximal or cornual occlusion. The incidence of false-positive results is estimated to be 50%.3 Hurd and colleagues reported that an apparent unilateral obstruction might be resolved in more than 50% of the patients by rotating the patient in a direction that places the obstructed tube in more inferior position.4
Pregnancy can occur after HSG. Perhaps, this is due to dislodging of a mucus plug or necrotic debris from the tubal lumen. In a randomized study, the pregnancy rate in women with patent tubes was 64% after HSG using oil-soluble contrast medium and 56% after the use of water-soluble contrast medium.5
Sonohysterosalpingography
Sonohysterosalpingography, also referred to as hystero-contrast-sonography or HyCoSy, is an alternative to HSG. The technique involves introduction of fluid into the uterine cavity. This is an outpatient procedure that usually lasts about 20 minutes. Saline solution is an echo-free contrast medium for assessment of the uterine cavity. The fallopian tubes can be evaluated by another contrast medium, such as air, albumin with micro-air bubbles, or galactose with micro-air bubbles. This contrast medium outlines the fallopian tube, giving a hyperechoic appearance.6
In a meta-analysis that included more than 1000 women, a similar rate of detecting tubal pathology was reported between sonohysterosalpingography and HSG or laparoscopy.7 Sonohysterosalpingography showed a false tubal occlusion in 10% of cases when compared to laparoscopy and chromopertubation. When sonohysterosalpingography was compared to HSG, a false-positive rate of 13% was found.
Laparoscopic Procedures
Laparoscopic Chromopertubation
This has been the gold standard for investigating tubal patency. Furthermore, laparoscopy permits direct visualization of the whole peritoneal cavity, including other pathology such as perihepatic adhesions (see Fig. 47-1B). Details of this procedure are reviewed in Chapter 44.
Transhydrolaparoscopy
This technique involves the use of a culdoscopic approach and the use of a small endoscope to explore the pelvic cavity. It is performed with the patient in the dorsal lithotomy position. Using saline solution as a distension medium, the posterior aspect of the uterus and tubo-ovarian structures are inspected. The saline instillation continues throughout the procedure to float the tubes and the ovaries. The advantage of this procedure is that it can potentially be used in an office setting. The disadvantage of this procedure is that it does not allow evaluation of the whole abdominal or pelvic cavity. The main concern of transhydrolaparoscopy is bowel injury (about 0.65%).8
Salpingoscopy
This is an endoscopic approach to visualize the intraluminal part of the fallopian tube. The procedure is usually done with a rigid salpingoscope.9 The salpingoscope is introduced into the abdominal cavity through the operating channel of the laparoscope. An atraumatic forceps in the secondary port is used to grasp and align the ampullary segment of the tube. The salpingoscope is then slowly advanced into the tube from the fimbrial end. The inner portion of the tube is visualized until the tubal ostium. Saline solution is used as the distension medium.
Salpingoscopic findings can be classified into five grades. Grade I refers to normal mucosal folds; in grade II, major folds are separated and flattened; grade III refers to the presence of a focal lesion (adhesions, polyps, or strictures); in grade IV, there are extensive lesions with either preservation or loss of the mucosal folds; and grade V is complete loss of the mucosal folds. The cumulative pregnancy rate is inversely related to the degree of tubal damage.10,11 Salpingoscopy can also be performed through transvaginal hydrolaparoscopy.12
Falloposcopy
This transvaginal endoscopic technique13 involves the use of an extremely narrow microendoscope (0.45 to 0.5 mm in diameter) for transcervical tubal cannulation using local anesthesia. The entire fallopian tube can be visualized. There are two techniques. The first (coaxial technique) is a hysteroscopic approach where a flexible guidewire enclosed in a soft catheter is introduced into the uterotubal ostium. The catheter and the guidewire are slowly advanced for a distance of approximately 12 cm or until resistance is encountered. The guidewire is removed and the falloposcope is introduced through the catheter. In a multicenter trial, it was found that 40% of normal tubes diagnosed on HSG had abnormalities observed on falloposcopy.14 This coaxial approach lacks a uniform scoring system and the image quality is poor. The second technique involves the use of a linear everting catheter by a transvaginal approach that does not require hysteroscopy.15 This procedure is also limited by image quality. Neither procedure is commonly used.
MANAGEMENT OF TUBAL INFERTILITY
Basic Principles of Tubal Surgery
At operative laparoscopy, dissection is better performed using sharp dissection with minimal use of electrical or laser energy. Thermal damage is associated with higher risk of adhesion formation. The use of sutures should be limited as well. However, if needed the suture material should be fine and nonreactive (e.g., 6-0 polyglactin or polyglycolic acid). The sutures should be placed without strangulating the tissue. Hemostasis is achieved using microbipolar forceps.
Proximal Tubal Occlusion
Proximal tubal occlusion is found in 10% to 25% of women with tubal disease. It is mainly due to salpingitis isthmica nodosa. Other causes of failed filling of the tubes are chronic pelvic infection, congenital malformation, and tubal spasm. Tuberculosis may cause varying degrees of tubal damage from minimal to extensive proximal tubal block.16 The thick muscular wall of the proximal tube, with its physiologic sphincter and its narrow lumen, makes it susceptible for “obstruction” by mucous debris.17
Selective Salpingography and Tubal Catheterization under Fluoroscopy
This is an established procedure for diagnosis and treatment of proximal tubal occlusion (Fig. 47-2). The procedure is performed by passing a catheter through the cervix into the proximal tubes. Radiocontrast medium is then injected under fluoroscopic guidance. Similar to HSG, the pressure induced by the injection may help in overcoming the obstruction. Otherwise, a guidewire is introduced into the fallopian tube to overcome the obstruction.
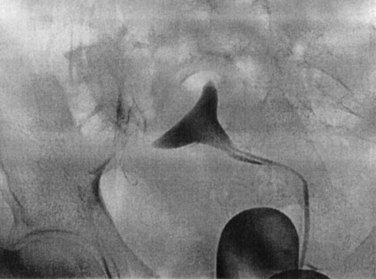
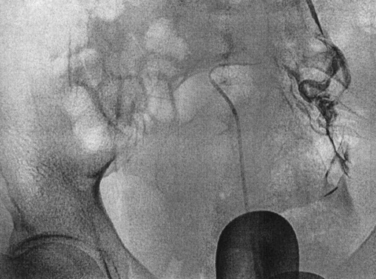
The procedure is usually performed under paracervical block with or without intravenous sedation. The first catheter is introduced through the cervix into the uterine cavity. A balloon is inflated to occlude the cervix. The second (ostial) catheter is then passed through the central lumen of the cervical catheter and advanced to the uterine cornua. Radiopaque contrast medium is injected into the tube directly (Fig. 47-3). Repeated radiographs are done to demonstrate the filling of the tube proximally and distally and whether peritoneal spillage occurs.
If selective salpingography is not successful, the third (uterine cornual) catheter with a guidewire is used. Threading of an atraumatic guidewire through the catheter into the ostium and the isthmus (tubal cannulation) unblocks the obstruction. In most cases (85%), the tubal occlusion can be overcome. Yet, reocclusion rate is high (30%). Tubal perforation can occur in 3% to 11% of cases; however, it heals spontaneously without any further treatment. The pregnancy rate after selective salpingography and tubal catheterization is about 50% (Table 47-2). The procedure can be repeated if the tubes reocclude. If the procedure fails, patients can be offered IVF or reconstructive tubal surgery.
Table 47-2 Pregnancy Rates after Selective Tubal Catheterization
| Technique | Pregnancy Rate (%) | Ectopic Rate (%) |
|---|---|---|
| Fluoroscopic technique | 50% | 2–9% |
| Hysteroscopic technique | 50% | 5% |
Hysteroscopic Transcervical Tubal Cannulation
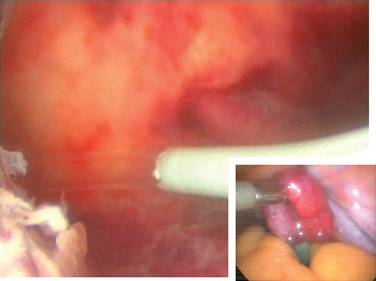
This hysteroscopic procedure is similar to selective salpingography and tubal catheterization. This procedure typically uses a Novy cornual cannulation set (Cook Ob/Gyn, Spencer, Ind.). A catheter is introduced into the working channel of an operative hysteroscope. The catheter is then advanced toward the tubal orifice and wedged against the ostium (Fig. 47-4). Dilute indigo carmine is then injected while observing laparoscopically for spillage from the fimbriated end of the tube. If there is no spill an inner catheter with a guidewire is then introduced. The guidewire is introduced through the uterotubal junction and then into the tube. Only then is the inner catheter introduced. No resistance should be met. The guidewire is then removed and dilute indigo carmine is injected.
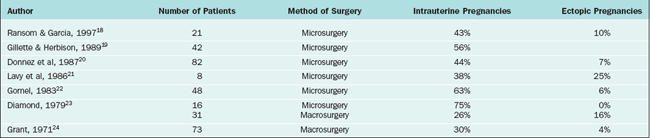
Microsurgical Resection and Anastomosis
The edges of the transected tube are examined under the microscope or close-contact laparoscope. Depending on the laparoscope and the distance between the end of the scope and the tissue, magnification up to 10-fold can be obtained. The two cut ends of the tube are approximated with several interrupted sutures of 6-0 polyglactin in the mesosalpinx. Three to four interrupted 7-0 sutures are then placed in the mucosa and muscularis layers circumferentially. The pregnancy rate following cornual anastomosis is approximately 50% (Table 47-3). A meta-analysis of different techniques found that the pregnancy rate after microsurgical repair of cornual obstruction is 58.9%, with an ectopic pregnancy rate of 7.4 %.25 Most patients choose IVF after failed cannulation techniques rather than a surgical approach.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


