Fig. 1 a–c
A 66-year old female patient after blunt abdominal trauma showing multiple, rounded, high-attenuation areas in the spleen on a arterial-phase computed tomography (CT) images, being only faintly visualized in b portal-venous-phase CT. c Selective splenic angiogram confirms pseudoaneurysm formation (arrowhead) in the upper pole of the spleen. The patient underwent subsequent proximal splenic artery embolization (not shown)
Liver
Traumatic hepatic injuries are common and can be readily diagnosed with CT. Besides liver contusions, characterized by periportal edema (or tracking) (Fig. 2a), lacerations are the most frequently identified injury in liver trauma. Lacerations are identified as predominately linear areas, often with a branching pattern, of relative hypoattenuation (Fig. 2b) [16]. Liver hematomas occur intraparenchymally, appearing as ill-defined hypoattenuating areas in the liver parenchyma; or subcapsularly, appearing as crescent-shaped hypoattenuating regions compressing the underlying liver segments. Additional important imaging findings that often guide treatment include injury to the major hepatic veins, presence of active bleeding into the peritoneal cavity, and presence of hemoperitoneum. Late complications include bile leak, biliary stricture, hepatic abscess, delayed hemorrhage, and other vascular complications [10].
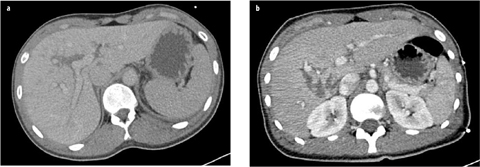
Fig. 2 a, b
a A 23-year-old female patient after blunt abdominal trauma with liver contusion predominantly affecting the right liver lobe, indicated by periportal edema (or tracking). b A 20-year-old female patient after blunt abdominal trauma with lacerations of liver segments I, VI, and VII
Pancreas
Blunt pancreatic trauma is an exceedingly rare but lifethreatening injury with significant mortality rates. CT findings of acute pancreatic trauma may be separated into direct and indirect features [17]. Direct signs include parenchymal laceration, transection, and focal enlargement or hematoma. Lacerations, which are further classified into superficial (involving <50% of the parenchymal thickness) and deep (involving >50% of the pancreatic parenchyma), manifest as linear, irregular, low-attenuation areas within the pancreatic parenchyma (Fig. 3). Disruption of the main pancreatic duct is more likely in deep lacerations and complete transections compared with superficial lacerations [18]. Given that injury of the main pancreatic duct is the major determinant of patient out-come in pancreatic trauma, early diagnosis of pancreaticduct injury is crucial.
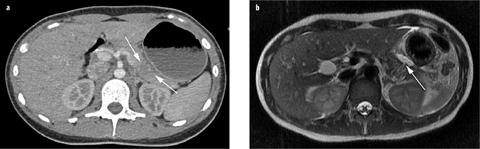
Fig. 3 a, b
A 21-year-old female patient after blunt abdominal trauma showing a deep (<50% of parenchymal thickness) transection (arrows) of the pancreas on computed tomography (CT). b Suspected main pancreatic duct injury was confirmed on T2-weighted magnetic resonance (MR) imaging, demonstrating the fracture line of the pancreas and a peripancreatic fluid collection (arrow)
Adrenal Gland
Traumatic adrenal injury occurs in <5 % of cases of blunt abdominal trauma and most commonly affects the right adrenal gland [19]. The most common CT feature of adrenal injury is a round or oval hematoma expanding the gland (Fig. 4) and is present in approximately 80% of adrenal trauma cases. Average hematoma size is 2–4 cm, and mean attenuation is 55 HU. Hematomas characteristically do not enhance after contrast media administration. Due to the uncommon nature of isolated adrenal injury, if an apparent isolated injury is seen, it is critical to search for other traumatic injuries of the abdomen.

Fig. 4
A 53-year-old male patient after blunt abdominal trauma showing an oval hematoma expanding the right adrenal gland (arrow) on computed tomography (CT) with a mean attenuation of 50 HU
Bowel and Mesentery
Injury to the hollow viscera and mesentery are rare, occurring in only 5% of patients who experience blunt abdominal trauma. At least one half of injuries to hollow viscera involve the small bowel, followed by the colon and stomach [20].
A variety of signs indicate bowel and mesenteric injury at CT, with some being sensitive and others being specific [10]. Therefore, the combination of findings increases the likelihood of a relevant injury. The specific signs of bowel injury include transection of the wall with focal discontinuity, pneumoperitoneum, and pneumoretroperitoneum.
Specific signs of mesenteric trauma include mesenteric hematoma, peritoneal extravasation of intravenous contrast-enhanced blood (Fig. 5), and abrupt termination or irregularity of the walls of mesenteric vessels. The more sensitive CT signs of bowel trauma include focal wall thickening, abnormal bowel wall enhancement, illdefined stranding of the mesentery, and free intraperitoneal fluid. Extraluminal gas is highly suggestive for bowel perforation, with a variable amount of free gas [21].
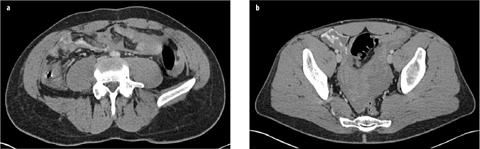
Fig. 5 a, b
 Enterography: Small Bowel Imaging That Impacts Patient Management
Enterography: Small Bowel Imaging That Impacts Patient Management
 to Perform and Report Magnetic Resonance Imaging for Pelvic Floor Dysfunction: An Interactive Case-Based Approach
to Perform and Report Magnetic Resonance Imaging for Pelvic Floor Dysfunction: An Interactive Case-Based Approach
 Should it Be Integrated into Screening and Clinical Routine Imaging?
Should it Be Integrated into Screening and Clinical Routine Imaging?
 Vascular Disease: Diagnosis and Therapy
Vascular Disease: Diagnosis and Therapy
 Abdominal Disease: Diagnosis and Therapy
Abdominal Disease: Diagnosis and Therapy
 Urography in Children
Urography in Children




A 19-year-old male patient with blunt abdominal trauma showing intraperitoneal extravasation of intravenous contrast-enhanced blood and extensive hemoperitoneum due to traumatic injury to the serosal layer of the ileum and mesenteric injury with traumatic transection of a segmental branch of the superior mesenteric artery
Related posts:
Enterography: Small Bowel Imaging That Impacts Patient Management
to Perform and Report Magnetic Resonance Imaging for Pelvic Floor Dysfunction: An Interactive Case-Based Approach
Should it Be Integrated into Screening and Clinical Routine Imaging?
Vascular Disease: Diagnosis and Therapy
Abdominal Disease: Diagnosis and Therapy
Urography in Children
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
