Fig. 13.1
Illustration of the human embryo at 8 weeks
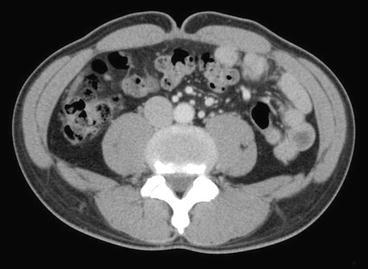
Fig. 13.2
Computed tomography image at the level of the umbilicus. There is no muscle layer or subcutaneous fat layer at the umbilicus
The deepest part of the umbilicus is the scar where the round ligament of the liver, the para-umbilical vein, and the urachus were once attached (Fig. 13.3). The fascia of the umbilical scar differs in structure from the linea alba, which is the site of fusion between the bilateral posterior layers of the rectus sheath [2–4].
Fig. 13.3
The deep surface of the umbilicus is the scar where the round ligament of liver, the paraumbilical vein, and the urachus are attached
The umbilicus, unique in shape, is also a key aesthetic landmark on the abdominal surface. The shape of the umbilicus varies from person to person. Most commonly, the umbilicus is either T-shaped or rounded. A crescent shape is common in obese persons, but the floor of even a crescent-shaped umbilicus is rounded, formed by the disk-shaped scar tissue.
13.2 Surgical Window to Access the Peritoneal Cavity
In conventional open surgery, laparotomy is performed without cutting out the umbilicus. Cutting the umbilicus has been avoided for very specific reasons: the risk of bleeding from umbilical vessels, the risk of surgical wound contamination and ensuing infection by bacteria harbored in the umbilicus, and the difficulty involved in reconstructing the umbilicus aesthetically. Laparoscopic surgery necessitates only small wounds for the trocars and a route for tissue extraction. Because of its anatomy, the umbilicus is the perfect candidate for a workable surgical access site. It meets the goal of reducing or eliminating the need for laparoscopic trocars and has made it easy for surgeons to improve outcomes [5] (Fig. 13.4).

Fig. 13.4
The single-incision multi-trocar method applied to laparoscopic cholecystectomy. The operation is completed strictly through the umbilicus
13.3 Surgical Window for Tissue Extraction
Due to its anatomical structure, the umbilicus is a suitable gate for extraction of the resected specimen. When the umbilicus is cut out, the incision is approximately 2 cm; however, the surgeon can extract a specimen that is as large as 4 cm in diameter by withdrawing it through the umbilicus. The simple structure of the umbilicus lends elasticity, which in turn facilitates the removal of a large specimen (Fig. 13.5). The incision should be sized according to the size of the specimen.
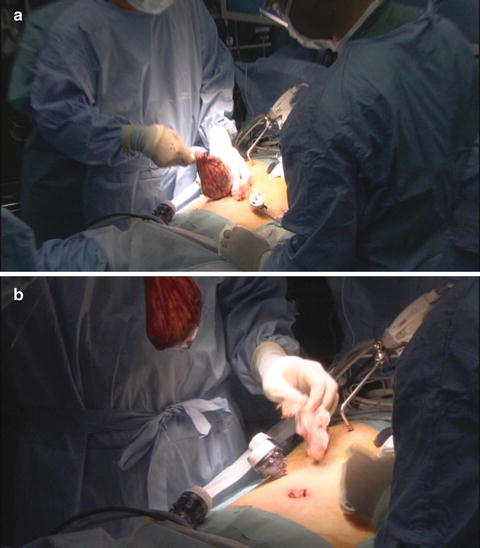
Fig. 13.5
The resected gastric specimen, together with dissected lymph nodes, is extracted through the umbilicus. The tissue is removed in a bag that, when packed, is 3–4 cm in diameter and pulled through the opened umbilicus
13.4 Methods for Single-Port Laparoscopic Surgery at the Umbilicus
There are two main single-port laparoscopic surgery (SPLS) methods: the single-incision multi-trocar method and the multi-channel port method [6]. The former is the original SPLS method. With this method, several trocars are placed in the same single incision. The advantages of this method are the ease of placing the trocars, the ease in manipulating the forceps even from the small single incision, and the fact that standard devices can be used. However, the single-incision multi-trocar method can be problematic. The procedure is not standardized, and proper placement of the trocars depends on the surgeon’s experience and skill level [5, 7].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


