Resection
Preservation
Optional resection
Organ
Pancreas (body/tail), left adrenal gland, gallbladdera, spleen
Stomach, duodenum
Vessels
Celiac artery, common hepatic artery, splenic artery, dorsal pancreatic artery, short gastric vessels, posterior gastric artery, inferior mesenteric vein.
Inferior pancreaticoduodenal artery, gastroduodenal artery (pancreatoduodenal arcades), proper hepatic artery, the right gastric and right gastroepiploic vessels, gastrocolic trunk
Portal vein, middle colic vessels. Left gastric arterya [30] and inferior phrenic arteries can be preserved based on the anatomical features.
Other tissues
Part of the crus of the diaphragm, the Gerota fascia, the celiac plexus and ganglions, the nerve plexus around the superior mesenteric artery, the retroperitoneal fat tissues bearing lymph nodes above the left renal vein, the transverse mesocolon covering the body of the pancreas
Right adrenal gland, bilateral kidneys
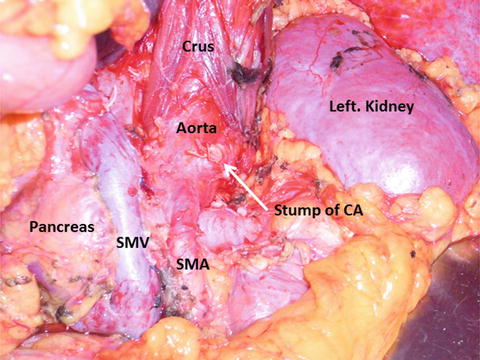
Fig. 16.1
The surgical field after the modified Appleby operation (DP-CAR). CA celiac axis, SMV superior mesenteric vein, SMA superior mesenteric artery
Indications for the Modified Appleby Operation (DP-CAR) in Patients with Pancreatic Body/Tail Carcinoma
The modified Appleby operation should be performed in institutions with well-trained and experienced staff. When it was initially introduced, this procedure was indicated for patients with pancreatic body/tail carcinoma involving the celiac axis and/or CHA (Fig. 16.2). Recent literature has reported that this procedure can be used for patients with pancreatic body/tail tumors that involve or approximate at least one of the common hepatic arteries, the root of the splenic artery, or the celiac axis [1] (Fig. 16.2). This finding implies that this procedure may also be indicated for resectable pancreatic body/tail carcinomas situated near the root of the splenic artery. Our investigation regarding the relationship between radicality and the distance between the edge of the tumor and the splenic artery root in patients who underwent standard DP revealed that microscopically positive margins were detected more frequently in patients with tumors situated ≤10 mm from the splenic artery origin than in those with tumors >10 mm from the origin of the splenic artery [30]. Therefore, we suggest that DP-CAR should be performed to obtain an R0 resection in patients with potentially resectable pancreatic body/tail carcinomas with tumors located ≤10 mm from the splenic artery origin.
Fig. 16.2
The association between the category of resectability and the tumor abutment of the celiac axis and its branches with imaging of computed tomography. SA splenic artery, CHA common hepatic artery, CA celiac axis
Our study also demonstrated that the overall survival rate of patients with no histopathologic evidence for invasion of either the portal venous system or artery (double-negative invasion) was greater than that of other patients. With regard to artery invasion, Kanda and colleagues [31] reported that invasion of the splenic artery is a crucial prognostic factor in patients with carcinoma of the body/tail of the pancreas. Moreover, extended pancreatectomy with major arterial resection did not result in long-term survival in previous reports [32–38]. Therefore, we carefully evaluated the patients with double-negative invasion into the portal venous system and the arterial system by preoperative imaging to determine indications for DP-CAR. However, the diagnostic accuracy of even the most sensitive modern imaging techniques is not equivalent to that of the microscope. Radiographic abutment of tumor and vessel does not necessarily indicate true vascular invasion.
The Role of the Appleby Operation and Arterial Resection
Recent studies have reported that arterial en bloc resection in patients undergoing pancreatectomy for pancreatic cancer is associated with poor short- and long-term outcomes. These studies indicate that arterial resection may yield overall survival durations comparable to those obtained with standard resection and better than those observed following palliative bypass [12, 33, 34]. However, arterial resection is associated with significantly higher morbidity and mortality rates, which limit the oncological benefit of operations in which it is used [32]. In general, we conclude that arterial en bloc resection may be justified in highly selected patients owing to the potential survival benefit compared to resection, but that these patients should be treated within the bounds of clinical trials and within the context of a multimodality strategy [32–34].
The ability of the modified Appleby operation to achieve wider surgical margins relative to a standard DP is viewed as a potential benefit of the operation. In many borderline resectable cancers of the pancreatic head, the carcinoma abuts the superior mesenteric artery. This artery and the nerve plexus around it represent an absolute anatomic boundary of the surgical dissection. However, the modified Appleby procedure can extend the clearance of the surgical margin wider than it otherwise might be achieved using standard DP by enhancing the depth of dissection, behind the tumor by taking the aortic surface as a boundary. Another advantage of this procedure is the ability to relieve the cancer pain by celiac axis en bloc resection combined with removal of the tumor infiltrating plexuses. Recent studies have reported resolution rates of cancer pain after this procedure as high as 86–100 % [1, 12, 13] and improved quality of life after the procedure. The nutritional status and quality of life of the patients after this surgery were well maintained, and planned adjuvant therapy was generally received [39].
Preoperative Preparation for the Modified Appleby Operation (DP-CAR)
Several investigators have reported performing the modified Appleby operation without preoperative coil embolization of the CHA [13]. However, embolization has been suggested to decrease the risk of ischemia-related complications. The safety and efficacy of preoperative coil embolization still needs to be evaluated in clinical trials so its necessity remains controversial.
Preoperative coil e mbolization of the CHA requires collaboration between the surgeon and the interventional radiologist. The surgeons should precisely describe the planned ligation/division site, and the radiologist should place the coil appropriately to avoid coil migration into the arteries that are intended to be preserved [40, 41]. The diameter of the inferior pancreaticoduodenectomy is usually increased by about 1.5–2 times by the procedure.
Preparation of Instruments for the Modified Appleby Operation (DP-CAR)
The surgical instruments used in the modified Appleby operation (DP-CAR) are similar to those of ordinary pancreatic resection. The aortic clamps should be prepared in case of injury or a short ligation margin of the celiac trunk. Doppler ultrasonography should be performed routinely to evaluate intrahepatic arterial and portal flow.
The Procedure and Pitfalls of the Original Appleby Operation (DP-CAR)
The specific procedure we use for DP-CAR is as follows. First, the right gastroepiploic artery/vein and right gastric artery/vein are encircled by vessel tapes and preserved. Before the neck of the pancreas is transected, the bifurcation of the gastroduodenal artery (GDA) and the CHA is exposed, followed by exposure of the origin of the PHA. Confirmation that the periarterial nerve plexus around the bifurcation is negative for cancer cell infiltration should be performed using frozen samples to evaluate resectability in patients whose tumor is adjacent to this region. Kocher’s maneuver should be performed in case of accidental bleeding from the portal venous system. The gastrocolic trunk is preserved for venous return from the stomach. Transection of the pancreas is performed at a site sufficient to resect a margin of normal tissue to reduce the likelihood for cancer cell infiltration. In a patient whose tumor involves the portal vein, the resection and reconstruction of the portal vein are performed antecedently. After pancreatic transection, the dissection of the retroperitoneum must be performed from the right to left side in the manner of a radical antegrade modular pancreatosplenectomy procedure because the surgical field will be better and safer for the surgeon and assistants in case of bleeding [42]. By en bloc dissection of the lymph nodes around the CHA, the right celiac ganglion and celiac nerve plexus, as well as the origin of the celiac axis are exposed. Blood flow through the PHA, the right gastric artery, and the right gastroepiploic artery can then be confirmed by palpation; the intrahepatic arterial flow can also be checked by intraoperative Doppler ultrasonography after clamping the end of the CHA in patients who have undergone preoperative embolization of the CHA. The CHA is divided just proximal to the origin of the GDA (Fig. 16.3). In cases with dog-leg branching of the PHA and GDA, great care must be taken to preserve both arteries by avoiding ligation of bifurcation site (Figs. 16.4 and 16.5). By lifting the cut end of the distal pancreas and the CHA to the left, the superior mesenteric artery (SMA) can be dissected from the surrounding lymph nodes and nerve plexus toward its origin. Great care should be taken to preserve the inferior pancreaticoduodenal artery (IPDA) arising from the SMA or the first jejunal artery. The origin of the celiac axis is identified circumferentially just above the aorta and is divided. The origin and the direction of inferior phrenic arteries should be carefully noted in dissecting around the celiac axis in front of the aorta (Fig. 16.6).
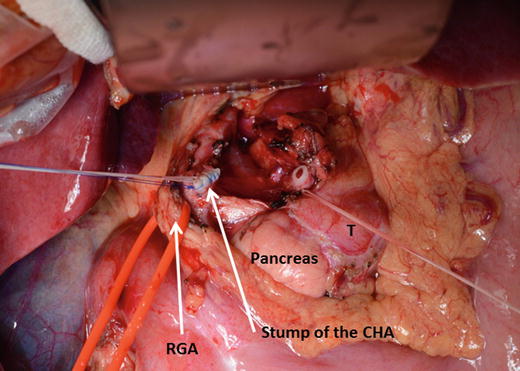
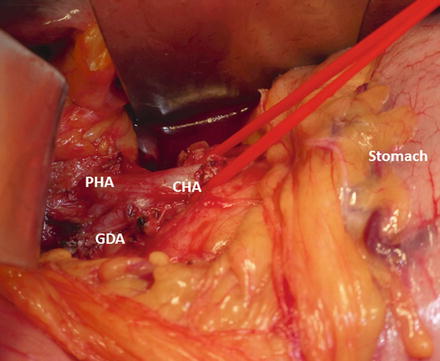
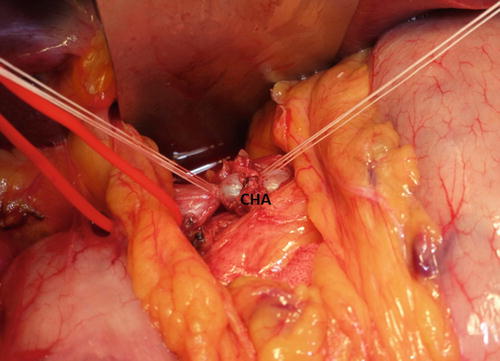
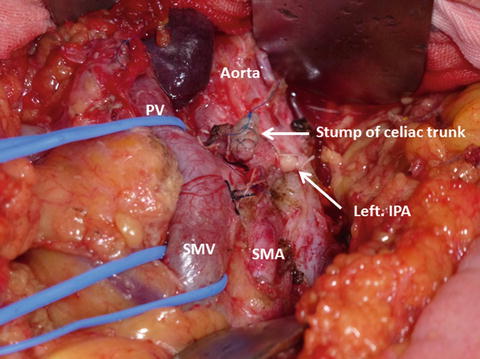
Fig. 16.3
The common hepatic artery was divided just proximal to the origin of the gastroduodenal artery. T pancreatic adenocarcinoma, CHA common hepatic artery, RGA right gastric artery
Fig. 16.4
In cases with “dog-leg” branching of proper hepatic artery and gastroduodenal artery, great care must be taken to preserve both arteries by avoiding ligation of the bifurcation site. CHA common hepatic artery, PHA proper hepatic artery, GDA gastroduodenal artery
Fig. 16.5
The common hepatic artery was ligated in the distal side. Pulsation within the proper hepatic artery and gastroduodenal artery was confirmed again after ligation. CHA, common hepatic artery
Fig. 16.6
The origin and the direction of inferior phrenic arteries should be carefully noted while dissecting around the celiac axis in front of the aorta. PV portal vein, SMV superior mesenteric vein, SMA superior mesenteric artery, IPA inferior phrenic artery
Postoperative Complications After Modified Appleby Operation (DP-CAR)
The rates of morbidity following this procedure are high as shown in Table 16.2. The presence of postoperative hemorrhage from the resected stump of the CHA due to a pancreatic fistula after DP-CAR is difficult to rescue by interventional radiology techniques. Therefore, a novel procedure to reduce the risk of pancreatic fistula formation is urgently needed for DP-CAR, especially in patients with thick pancreatic parenchyma [43, 44].
Table 16.2
Postoperative complications after DP-CAR
Author (Reference) | Reported year | Number of cases (n) | MSTa (month) | 1-year survival rate (%)a | Ischemia-related complication (%)b | Morbidity (%) | Mortality (n) |
|---|---|---|---|---|---|---|---|
Hishinuma, et al. [11] | 2007 | 7 | 19 | 30 | 0 | 29 | 0 |
Hirano et al. [1] | 2007 | 23 | 21 | 42 | 13c | 48 | 0 |
Wu et al. [12] | 2010 | 11 | 14 | 9 | 0c | 36 | 1 |
Takahashi et al. [13] | 2011 | 16 | 10 | 35 | 0c | 56 | 1 |
Yamamoto et al. [14] | 2012 | 13 | 21 | 25 | 38c | 92 | 0 |
Okada et al. [30] | 2013 | 16 | 25 | 42 | 6 | 44 | 0 |
DP-CAR may also be associated with gastric or hepatic ischemia. In several institutions, total gastrectomy is added if severe ischemia of the stomach is observed during the operation and if the surgeon cannot exclude the possibility of future necrosis of the remnant stomach. Unplanned arterial reconstruction is required in patients with accidental injury [1]. The sequelae of ischemic gastropathy include irregular, shallow, and wide ulcerations in the cardia of the stomach and/or symptoms of delayed gastric emptying; gastropathy may directly effect postoperative recovery and the schedule for adjuvant chemotherapy. With regard to hepatic ischemia, recent studies have reported a low incidence of clinically relevant hepatic infarction, and abnormal liver function usually resolves after several days. Necrotic cholecystitis due to spasms of the GDA and/or PHA has been reported. Although there is no clear evidence that preoperative embolization of the CHA reduces risks of ischemia, preoperative angiography should be performed to elucidate the arterial anatomy.
The greatest concern following the removal of the plexus around the celiac axis and the superior mesenteric artery is diarrhea, because it can influence nutritional status and quality of life. In many studies, diarrhea can be controlled by medication well eno ugh to maintain quality of life and nutritional status, usually with loperamide hydrochloride and rarely with tincture of opium [1].
Feasibility and Safety Compared to Standard Distal Pancreatectomy
The mean operative time associated with DP-CAR is significantly longer than that associated with standard DP due to the extended dissection and radical dissection required in the former; however, no differences with regard to mean estimated blood loss or mean postoperative hospital stay between the two procedures have been identified. In terms of postoperative complications, previous studies have reported the incidence of postoperative pancreatic fistula [45] and revealed no significant differences between the modified Appleby operation and standard distal pancreatectomy; however, delayed gastric emptying (DGE) was more common in the modified Appleby operation. Otherwise, mortality has been reported to be low in the recent literature [46] (Table 16.2).
Preservation of the LGA
Despite the favorable surgical outcomes described recently, DGE or ischemic gastropathy after the modified Appleby operation (DP-CAR) remains a common and frustrating complication. The incidence of DGE induced by ischemic gastropathy ranges from 13.0 and 30.8 % in published series [1, 14]. It is not a life-threatening complication, but it may result in a prolonged hospital stay and leads to a decreased quality of life, poor nutritional status, and delayed administration of postoperative adjuvant chemotherapy. In a recent study, several patients underwent combined total gastrectomy to prevent gastric ischemic complications during the modified Appleby operation (DP-CAR) [1, 14].
The LGA develops as the first branch of the celiac trunk embryologically, and it may branch antecedently in 68–72 % of cases as described above [25, 26]. The procedures used for the modified Appleby operation (DP-CAR) routinely include en bloc resection of the LGA [1], although cancer of the pancreas body requiring DP-CAR may not involve the LGA or the nerve plexus that surrounds it. We therefore attempt to preserve the LGA in patients whose LGA branches antecedently and in whom the distance between the LGA and carcinoma is more than 10 mm.
To clarify whether LGA preservation in DP-CAR (modified DP-CAR) could reduce the incidence of DGE and other postoperative complications, the medical records of 37 consecutive patients who underwent DP-CAR were evaluated for the incidence of DGE [47]. 23 patients (62 %) had LGA-resecting DP-CAR (conventional DP-CAR) and 14 patients (38 %) underwent distal pancreatectomy with resection of the CHA and splenic artery, with preservation of the LGA (modified DP-CAR) for pancreatic carcinoma. The patients with tumors situated more than 10 mm away from the antecedent branching LGA underwent modified DP-CAR (Fig. 16.7a–c). The antecedent branching of the LGA was found in 19 patients (51 %) in this study. In the conventional DP-CAR group, the LGA was involved in 20 patients (87.0 %). Clinically relevant DGE rates were 30 % in the conventional DP-CAR group, and 0 % in the modified DP-CAR group (p = 0.035). The R0 rate was higher in the modified DP-CAR group (79 %) compared to the conventional DP-CAR group (43 %) (p = 0.048). Univariate and multivariate analyses demonstrated that resection of the LGA was an independent risk factor for increased incidence of DGE (Table 16.3). Therefore, modified DP-CAR significantly reduced the incidence of DGE in comparison to conventional DP-CAR [47].
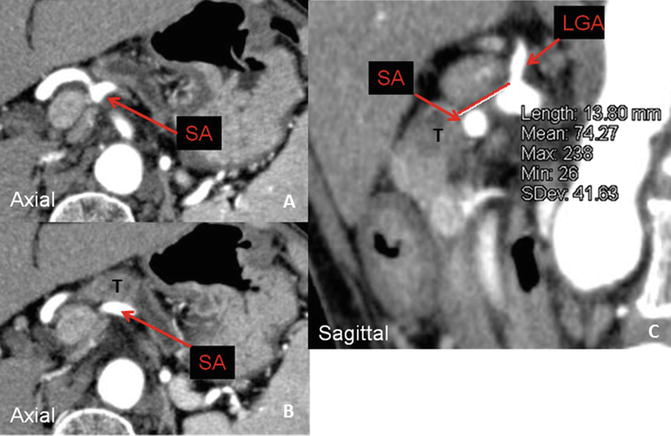
Fig. 16.7
 Overview of Multimodality Therapy
Emerging Systemic and Targeted Therapies
Overview of Multimodality Therapy
Emerging Systemic and Targeted Therapies
 Palliative Operations for Unresectable Pancreatic Cancer
Palliative Operations for Unresectable Pancreatic Cancer
 Role of Radiation Therapy
Role of Radiation Therapy
 Surgical Approach to Borderline Resectable Tumors of the Left Pancreas
Surgical Approach to Borderline Resectable Tumors of the Left Pancreas
 Endoscopic and Percutaneous Biliary Drainage Procedures: Role in Preoperative Management, Diagnosis, and Palliation
Endoscopic and Percutaneous Biliary Drainage Procedures: Role in Preoperative Management, Diagnosis, and Palliation




Patients with tumors situated more than 10 mm away from the antecedent branching left gastric artery undergo distal pancreatectomy with resection of the common hepatic artery and splenic artery, with preservation of the left gastric artery (modified DP-CAR) at our institution. (a) An axial image shows the root of the splenic artery. (b) An axial image reveals tumor abutment of the splenic artery. (c) A sagittal image shows that the distance between the tumor and the left gastric artery was 13.8 mm in this case. SA splenic artery, LGA left gastric artery
Related posts:
Overview of Multimodality Therapy
Emerging Systemic and Targeted Therapies
Palliative Operations for Unresectable Pancreatic Cancer
Role of Radiation Therapy
Surgical Approach to Borderline Resectable Tumors of the Left Pancreas
Endoscopic and Percutaneous Biliary Drainage Procedures: Role in Preoperative Management, Diagnosis, and Palliation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
