Figure 1.1
Contrast-CT of the abdomen. The dotted line shows the schematic pathway of intraperitoneal laparoscopic left nephrectomy. However, this curved line is in reality straightened by the lateral position of the patient lying on the opposite side and the fall of the colon medially after Toldt’s fascia is incised
The renal arteries arise laterally from the aorta at L2 level, immediately below the origin of the superior mesenteric artery. Renal artery originating from the level of L1–L2 intervertebral disc has been observed in 37.0 % and 38.9 % of cases on the right and left sides, respectively [2]. The right renal artery courses behind the inferior vena cava to join the corresponding kidney while the left renal artery joins directly the left kidney. At the renal hilum, they lie between the renal veins anteriorly and the renal pelves posteriorly; the mnemonic VAP (Vein-Artery-Pelvis) refers to this topography from anterior to posterior. The left renal vein crosses the aorta anteriorly to join the vena cava. During its course, it passes between the aorta and the first few centimeters of the superior mesenteric artery (SMA) originating from the anterior aspect of the aorta (Fig. 1.2). This position exposes the left renal vein to the rare entrapment or nutcracker syndrome between the aorta and the SMA. The left renal vein is typically longer than the right measuring 6–10 and 2–4 cm respectively. This is the reason why the left kidney is more frequently preferred for a transplantation procedure. The left renal vein receives the left adrenal vein superiorly, one or two lumbar veins posteriorly, and the left gonadal vein inferiorly, while its right counterpart does not receive any tributaries. Anatomical variations of the renal vasculature are common, occurring in 25–40 % of kidneys, and may exist in multiple renal arteries (up to 5!) mostly on the left side [1], and retroaortic (Fig. 1.3) or circumaortic left renal vein. It is not uncommon to see a lumbar vein joining the gonadal vein just before it enters the renal vein. Supernumerary veins are less commonly encountered, and occur mostly on the right side. It is also common to see early division of the renal arteries. More rarely found is a precaval right renal artery and a duplicated Inferior Vena Cava [3] (Fig. 1.4). When lower pole arteries are present, it is of surgical importance to remember their tendency to cross anterior to the IVC on the right side and anterior to the collecting system on either side, eventually causing a pelvi-ureteric junction obstruction.
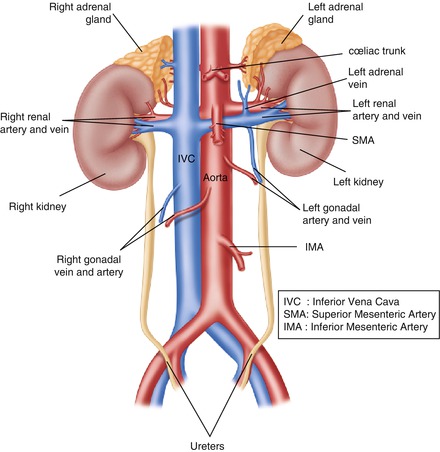




Figure 1.2
Retroperitoneum: kidneys, ureters, adrenals and great vessels
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
