Fig. 21.1
(a) ESD: Mucosa, with some submucosal tissue, is resected, and the exposed muscle layer facilitates as a barrier to esophageal content. (b) POEM: Muscle layer was dissected in submucosal tunnel. Mucosa works as a barrier between esophageal lumen and mediastinum. (c) POET: Tumor from muscle layer was resected through submucosal tunnel. Mucosa acts as a barrier to avoid mediastinitis
The POEM Procedure
Equipment Required for POEM
Endoscope and Distal Attachment
A standard forward-viewing diagnostic gastroscope can be used for the POEM procedure. But if it is available, a large working channel (3.2 mm) endoscope with water jet function is more useful. A transparent distal small “tapered” cap (ST Hood; Fujifilm, Tokyo, Japan) is preferably attached at the tip of the endoscope. An oblique cap (MH-588; Olympus, Tokyo, Japan) can be used as an alternative. The oblique cap is particularly necessary for clipping the esophageal opening. An overtube is used for stabilization of the endoscope which effectively avoids mucosal laceration at the mucosal incision site during the POEM procedure. This equipment used for POEM is similar to that used for ESD.
Carbon Dioxide (CO2) Insufflator
CO2 as insufflation is essential to achieve a safe POEM. Endoscopic CO2 insufflation with a controlled gas feed of 1.2 L/min is beneficial for reducing the risk of both mediastinal emphysema and pneumoperitoneum. Air supply button should definitely be closed during the POEM procedure, even when CO2 insufflator is turned on. In contrast, ESD can be carried out even under air insufflation, because the muscle layer is definitely kept intact.
Triangle-Tip Knife
A triangle-tip knife (TT knife) (KD-640L; Olympus) is used for submucosal tunneling and myotomy. The TT knife has a triangle plate at its tip. The Triangle plate has three angulations that allow spraying of energy toward a wide circumferential range. Submucosal dissection is effectively carried out without making direct contact with the tissue to be dissected.
Electrocautery Generator
A high-frequency electrosurgical energy generator (VIO300D; ERBE Elektromedizin GmbH, Tubingen, Germany, or ESG400; Olympus, Tokyo) that has a spray coagulation mode with non-contact tissue dissection is effectively used in combination with the TT knife. Spray coagulation mode, effect 2, 50 W is the best match with the TT knife for both submucosal dissection and myotomy. Settings should be individually adjusted during the operation.
Coagulation Forceps
Monopolar coagulating forceps (Coagrasper, FD-411QR; Olympus) are used for hemostasis and coagulation of large vessels, when encountered during dissection. The preferred electrocautery setting is soft coagulation 80 W, effect 2.
POEM Procedure
The following technical details of the POEM procedure have consistency from original report [24–27] (Fig. 21.2).
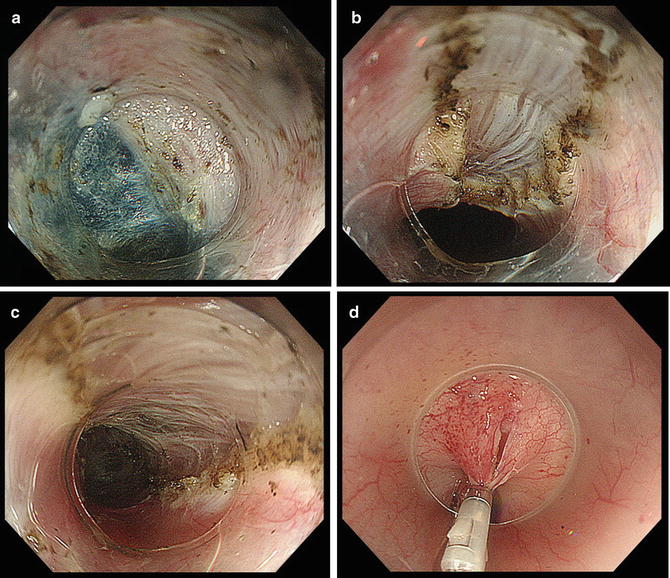
Fig. 21.2
Endoscopic images of POEM. (a) Submucosal tunnel. Submucosal dissection is made along the surface of the circular muscle layer. In this image, the top half is the muscle layer surface and the bottom half is the submucosal layer stained with indigocarmine. (b) Myotomy started. Myotomy begins at 2 cm distal from mucosal incision. Selective circular myotomy is intended in order to avoid mediastinal injury. (c) Completion of myotomy. Cut ends of circular muscle stay apart, resulting in good relaxation of the LES. (d) Closure of mucosal incision. Mucosal incision is closed with regular hemostatic clips. Complete closure of mucosal incision is confirmed by endoscopic vision
Step 1: General Anesthesia and CO2 Insufflation Through Endoscope
POEM is performed under general anesthesia with endotracheal intubation, keeping the patient in the supine position. CO2 insufflation is absolutely mandatory to perform a safe POEM procedure. CO2 insufflation theoretically avoids pneumomediastinum and air embolization. It is extremely important to check that the air feed button on the endoscopy unit remains closed, repeatedly throughout the entire procedure, even when the CO2 insufflation switch is turned on. If air was insufflated, it could cause catastrophic complications. To prevent abdominal compartment syndrome, the upper abdomen is checked periodically during the procedure. When the abdomen is excessively distended, abdominal wall puncture will be performed using an injection needle so as not to develop into abdominal compartment syndrome.
Step 2: Submucosal Tunneling
After injection of normal saline with indigo carmine dye, a 2-cm longitudinal incision is created on the anterior wall. Submucosal tunnel is generally created at anterior wall with one-third circumferential dissection of the esophageal lumen.
Myotomy at 2 o’clock direction, continuing toward lesser curve of stomach, potentially avoids damage to the sling collar muscle that is the major component of His angle. His angle is considered a natural anatomical barrier to postoperative GERD. The estimated length of the submucosal tunnel, although individualized, becomes approximately 16 cm (from 29 to 45 cm from patient’s teeth). If patients have abnormal contractions of the upper esophagus, myotomy is extended toward proximal side. The longest myotomy performed at Northern Yokohama Hospital was 25 cm.
Step 3: Endoscopic Myotomy
Dissection of the circular muscle bundle is usually started at the level of 2 cm distal to the mucosal entry point in submucosal tunnel. The standard length of myotomy is more than 10 cm (average 13 cm). A TT-knife permits selective dissection of the inner circular muscle layer, which potentially avoids incidental damage to the mediastinal critical organ. In other words, preserved longitudinal muscle layer is the safety margin of myotomy. All processes can be done with direct endoscopic visual control, and careful dissection is the simplest way to maintain safety. If during initial myotomy the thickness of the circular muscle cannot be predicted, it is advisable to begin myotomy by careful step-by-step dissection until the longitudinal muscle layer is identified at the bottom of the myotomy site. Even though the outer longitudinal muscle layer has been preserved, it is thin enough to split just by CO2 insufflation or even subtle touch of endoscopy on it.
Circular muscle dissection advances from proximal to distal, maintaining the correct dissection plane. The myotomy is extended to a distance of 2 cm toward the stomach. Myotomy at the narrow gastroesophageal junction (GEJ) has a higher risk of incidental mucosal damage, though repeated submucosal injection may work as a cushion and potential way to avoid damage. Smooth passage of the endoscope through the GEJ at the end of myotomy provides immediate confirmation of complete myotomy. At the LES, particular attention should be paid to ensuring that all circular muscle bundles responsible for achalasia are completely cut.
In laparoscopic Heller myotomy, the surrounding structures (phrenoesophageal ligament) of distal esophagus need to be dissected to expose the abdominal esophagus. This dissection causes potential hiatal hernia resulting in severe post-surgical GERD. In order to prevent it, a partial antireflux procedure, such as Dor fundoplication, is routinely performed. In contrast, no antireflux procedure is added after the POEM procedure, because the original hiatal attachments and the acute angle of His are left untouched and the flap-valve mechanism is kept intact.
Another major advantage of POEM is the flexibility of myotomy length. In POEM, myotomy is routinely made more than 10 cm, with at least 1 cm cut to gastric side. In laparoscopic surgery, a limited length with a maximum of 10 cm is capable to be performed because there is limited exposure of the distal esophagus under laparoscopic vision. In cases with vigorous achalasia or diffuse esophageal spasm, long myotomy is recommended. In POEM, the direction of myotomy can also be flexibly set. In cases of previous surgical failure, posterior myotomy is recommended to avoid access to the scar site from previous surgical myotomy.
Related posts:
 Management of Gastrointestinal EMR and ESD Perforation: From Lab to Practice
Management of Gastrointestinal EMR and ESD Perforation: From Lab to Practice
 Submucosal Fluid Cushion Injection Fluid: Western Perspective
Submucosal Fluid Cushion Injection Fluid: Western Perspective
 Regenerative Medicine for Stricture Management: What does the Future Hold?
Regenerative Medicine for Stricture Management: What does the Future Hold?
 Advanced Endoscopic Imaging in the Upper Gastrointestinal Tract
Advanced Endoscopic Imaging in the Upper Gastrointestinal Tract
 Endoscopic Submucosal Dissection for Superficial Esophageal Cancer
Endoscopic Submucosal Dissection for Superficial Esophageal Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


