Chapter 36 Stones in the bile duct
Endoscopic and percutaneous approaches
Historical Overview
In the 1970s and 1980s, endoscopic retrograde cholangiopancreatography (ERCP) transformed the diagnostic approach to suspected biliary disease and jaundice (see Chapters 18 and 27). Similarly, in the years since it was first performed in humans (Classen & Demling, 1974; Kawai et al, 1974), endoscopic sphincterotomy (ES) has had a dramatic impact on the management of biliary disease, specifically in the treatment of common bile duct (CBD) stones. Approximately 150,000 endoscopic biliary sphincterotomies are performed annually in the United States, and the availability of this procedure undoubtedly influences surgical decision making, when CBD stones are diagnosed on imaging or suspected, and when ERCP and ES are readily available. The surgical community initially resisted the introduction of ERCP and ES into CBD stone management, until their roles became established when they were shown to reduce the mortality rate significantly in a range of situations (Carr-Locke & Cotton, 1985; Cotton, 1984). Interest in ERCP and endoscopic sphincterotomy as definitive therapy for CBD stones grew in the 1990s after the introduction of laparoscopic cholecystectomy. Patient-related factors, clinical judgment, availability of expertise, and current evidence from clinical trials must be combined to decide on an endoscopic, percutaneous, or surgical approach. Although ERCP as a diagnostic modality has been replaced by noninvasive imaging modalities such as magnetic resonance cholangiopancreatography (MRCP; see Chapter 17), it remains the major nonoperative tool to manage biliary diseases such as CBD stones and obstructive jaundice.
Indications for Endoscopic Therapy
Patients with CBD stones may be seen initially with asymptomatic stones on noninvasive imaging or direct cholangiography or with a variety of clinical problems alone or in combination, such as cholestasis, pain, cholangitis, and pancreatitis (see Chapter 30). In the early days of ES—at a time when few endoscopy centers could offer the technique, and criticisms by surgical experts were common—it was considered justifiable only in elderly postcholecystectomy patients with recurrent or retained bile duct stones who were at high risk of serious complications from open surgical CBD exploration or reexploration (Blumgart & Wood, 1978). The impressive successes of ES in this group combined with expanded availability, a low rate of complications, and strong patient preference led many centers to widen their indications for the procedure to include younger and fitter postcholecystectomy patients and those with a gallbladder in situ. This change initially occurred in the absence of comparative trial data, and there was such enthusiasm for ES that the establishment of randomized trials was difficult, although nevertheless essential to clarify relative morbidity and mortality risks, as different groups of patients were likely to be treated empirically by endoscopic or surgical means and were not comparable (Cotton, 1984).
1 Acute cholangitis regardless of gallbladder status
2 Acute gallstone pancreatitis regardless of gallbladder status
4 Postcholecystectomy, stone shown on intraoperative cholangiogram
5 Postcholecystectomy, retained stone, early presentation
6 Postcholecystectomy, late presentation
7 Gallbladder in situ, variable risk factors for surgery, possible need for subsequent cholecystectomy
Endoscopic Techniques (See Chapter 27)
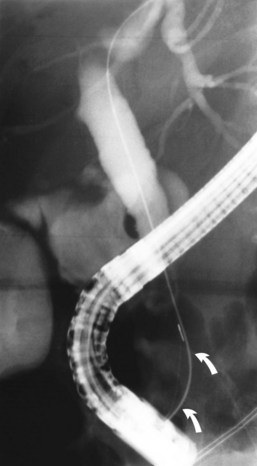
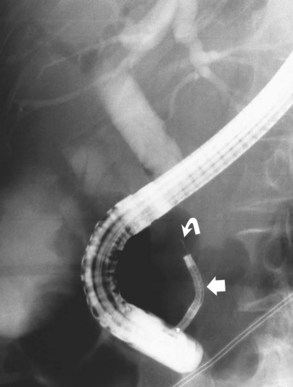
ES is usually the first therapeutic step and immediately follows diagnostic ERCP, which delineates the problem to be treated and allows accurate placement of instruments within the CBD. Standard pull-type sphincterotomes allow a vertical incision to be made from the papillary orifice in a cephalad direction along the intramural course of the CBD for a variable length (average, 10 to 15 mm) depending on local anatomy, the degree of CBD dilation, and the size of stone to be removed (Fig. 36.1). The incision is produced by the controlled application of monopolar electrocautery delivered by a generator specifically designed for endoscopic use, which does not exceed 150 W output. It is fundamental to good ES technique that complete control of wire tension and electrocautery be maintained at all times, whether the ES incision is made as a single continuous movement or in incremental steps. “Smart” generators incorporate a pulsed generator (Erbe, Tubingen, Germany; ConMed Endoscopic Technologies, Billerica, MA) with feedback-controlled power output, and there is potential for increased safety in avoiding a “zipper effect” and reducing pancreatitis and bleeding.
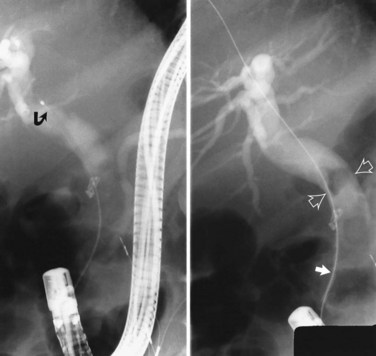
Radiographic confirmation of correct sphincterotome placement within the CBD is mandatory to avoid pancreatic trauma. Occasionally, a precut papillotomy, more appropriately called an access papillotomy, is needed to initiate ES when the standard instrument cannot be inserted deeply. This incision is often needed when cannulation has been prevented by an impacted stone. The needle-knife is more useful in this situation, because the intramural CBD is usually grossly distended and easily incised, starting from the papilla and extending cephalad. Needle-knife fistulotomy is a variant of this technique; the incision is begun above the papilla to form a choledochoduodenal fistulotomy. This technique is similar in efficacy to needle-knife papillotomy, but more often it requires mechanical lithotripsy, although it may have a lower rate of pancreatitis (Mavrogiannis et al, 1999). Patients with Billroth II partial gastrectomy (Fig. 36.2) and Roux-en-Y bypass operations present special problems to the endoscopist, and numerous methods have been described to obtain successful cannulation (Lin et al, 1999; Wright et al, 2002) and removal of CBD stones (Bergman et al, 2001).
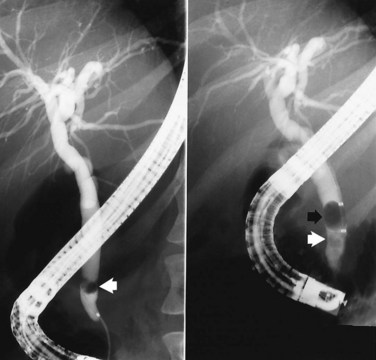
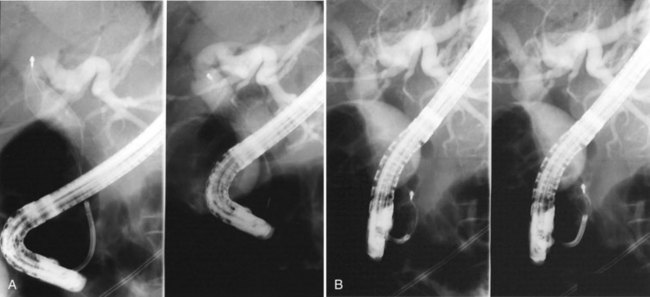
It is standard practice to attempt stone extraction from the CBD immediately after ES. The two accessory instruments used most commonly for this are the Dormia basket (Fig. 36.3) and the Fogarty balloon (Fig. 36.4), which are greater than 90% successful in clearing the CBD. It also is possible to extract stones without a preliminary ES using a balloon dilator (Fig. 36.5) (Bergman et al, 1997). Randomized trials of balloon dilation of the papilla compared with ES have shown similar outcomes for successful stone removal but an increased need for lithotripsy, and although the overall complication rates were similar, there was a higher rate of post-ERCP pancreatitis after balloon dilation if sphincterotomy was not performed beforehand (Baron & Harewood, 2004; Bergman et al, 1997; Disario et al, 2004). Large-diameter balloon dilation after sphincterectomy has become a popular and safe technique (Attasaranya et al, 2008).


Difficult Stones
The most difficult circumstances encountered during endoscopic stone removal result from technical difficulties with achieving deep biliary cannulation or in performing ES. These difficulties are sometimes because of an inaccessible papilla related to aberrant anatomy or unfavorable duodenal or papillary structures, such as a periampullary diverticulum, or prior surgery, such as Billroth II or Roux-en-Y reconstruction. Techniques have been described for the unique challenge of selective bile duct cannulation in a patient with a Billroth II partial gastrectomy (Lin et al, 1999). The performance of ES is also a challenge, because the visualized anatomy is inverted. In especially difficult cases, needle-knife sphincterotomy with a stent, nasobiliary drain, or guidewire used as a guide for cutting may be an option, or specially designed reverse-direction accessories. The literature on techniques of cannulation and sphincterotomy in Roux-en-Y reconstructions is limited (Wright et al, 2002), but some success has been reported with balloon enterosocopy or overtube-assisted ERCP (Koornstra et al, 2008, Kikuyama et al, 2009).
When ES has been successfully performed, extraction may be hindered by a variety of stone factors—including size, number, consistency, shape, and location of stones—ductal factors such as contour and diameter at the level of and distal to the stones, and the presence of coexisting pathology (e.g., stricture or tumor). Stones that are likely to be more difficult to extract and may require adjuvant techniques to remove them are those that appear larger than the endoscope on radiographic imaging (usually >15 mm); stones that are numerous or hard in consistency; stones that are square, piston shaped, or faceted that tightly fit the bile duct or that are packed against each other; intrahepatic stones; or stones located proximal to a stricture or narrowed distal bile duct or in a sigmoid-shaped duct. Techniques that have been developed to reduce stone size and facilitate endoscopic removal include mechanical lithotripsy, extracorporeal shock-wave lithotripsy (ESWL), intracorporeal lithotripsy with laser or electrohydraulic probes, and chemical contact dissolution therapy. Treatment options must be discussed jointly by the endoscopist, surgeon, and interventional radiologist when difficulties are encountered (Fig. 36.6; see Chapter 27).

Mechanical Lithotripsy
Removal of large CBD stones is a challenge for the most skilled endoscopist. Mechanical lithotripsy (see Chapter 27; Leung & Tu, 2004; Leung et al, 2001) remains the best initial option for stones that cannot be removed by conventional techniques, because it can be applied safely and effectively during the initial endoscopic procedure. Standard retrieval baskets contained within a polytef (Teflon) sheath may fail to crush large stones, because most exceed the breaking strength of the catheter. Standard-type, lithotripsy-compatible, and lithotripsy-convertible baskets are commercially available. Mechanical lithotripters are modifications of standard Dormia baskets and possess great tensile strength (Fig. 36.7). The reinforced basket is opened in the CBD, and the stone is entrapped within the braided wires. This procedure can be performed through the endoscope instrumentation channel, or it can be done after the endoscope has been removed from the patient and a metal sheath has been extended over the inner Teflon catheter. The end of the metal sheath is attached to a winding mechanism, which retracts the basket when cranked and impales the stone against the rigid distal end of the metal sheath leading to stone fracturing. The stone fragments can be removed with the same basket or a standard retrieval basket or balloon. In experienced centers, this technique allows removal of more than 90% of difficult bile stones that are refractory to standard extraction techniques (Chang et al, 2005; Shaw et al, 1993; Van Dam & Sivak, 1993).
Other Lithotripsy Modalities
For the 5% of patients with biliary stones resistant to ES and mechanical lithotripsy, other methods are available, including intracorporeal techniques (laser or electrohydraulic probes) and ESWL (Adamek et al, 1996). The choice between these methods or surgery depends largely on availability and local expertise.
Laser Lithotripsy
The first-generation laser systems using continuous wave energy neodymium:yttrium-aluminum-garnet (Nd:YAG) devices were ineffective at stone fragmentation and carried a high risk of thermal bile duct injury (Ell et al, 1988). Second-generation devices that have gained acceptance are based on high-energy, flashlamp, pulsed-dye laser technology. The application of the laser pulse leads to rapid expansion and collapse of a plasma on the stone surface, resulting in a mechanical shock wave. Initially, the only means to ensure laser-stone apposition was through the use of “mother and baby” dual endoscope systems (Cotton et al, 1990; Neuhaus et al, 1992a; Ponchon et al, 1991), but more recently, laser lithotripsy has been possible under fluoroscopic guidance with the use of devices that recognize the difference between stone and tissue. Two randomized trials comparing the xenon flashlamp pulsed rhodamine 6G laser with an integrated stone-tissue detection system with ESWL showed similar or improved efficacy in stone clearance, requiring fewer fragmentation and endoscopic sessions with use of the laser (Jakobs et al, 1997; Neuhaus et al, 1998).
Electrohydraulic Lithotripsy
Since its development during the 1950s in the former Soviet Union as a method to fragment rocks during mining, electrohydraulic lithotripsy has been adapted for medical use in the treatment of nephrolithiasis and, more recently, biliary tract calculi. The electrohydraulic probe consists of two coaxially isolated electrodes at the tip of a flexible catheter, which is capable of delivering electric sparks in short, rapid pulses leading to sudden expansion of the surrounding liquid environment and generating pressure waves that result in stone fragmentation (Picus, 1990). Stone contact with the electrode is achieved through the use of basket or balloon catheter systems (Siegel et al, 1990; Arya et al, 2004) or under direct visual targeting (Fig. 36.8) through the working channel of a daughter endoscope (Hixson et al, 1992), minimizing the risk of CBD injury and perforation. Reports document complete stone clearance after multiple sessions in 86% of patients (Adamek et al, 1996; Hixson et al, 1992; Siegel et al, 1990; Arya et al, 2004), and in a prospective nonrandomized trial, electrohydraulic lithotripsy was comparable to ESWL in stone clearance (Adamek et al, 1996). Its main advantages over laser lithotripsy are its lower cost and increased portability.
Extracorporeal Shock-Wave Lithotripsy
ESWL with a variety of lithotripsy machines is now an accepted alternative to endoscopic fragmentation of difficult bile duct stones. In contrast to intracorporeal techniques, direct contact with the stone is unnecessary. Most centers localize stones with fluoroscopic focusing during contrast perfusion of the bile duct through an endoscopically placed nasobiliary catheter or percutaneous drain (Gordon et al, 1991; White et al, 1998). Ponchon and colleagues (1990) reported ESWL success with an ultrasound localization system, although it was less effective when multiple stones were present. Several large series (Bland et al, 1989; Gilchrist et al, 1997; Sackman et al, 2001; Sauerbruch & Stern, 1989) indicated success rates for ESWL stone fragmentation of 53% to 91% and duct clearance in 58% to 90%. Minor complications are common and include hematuria, biliary pain, hemobilia, transient liver function test elevations, and cutaneous petechiae. Overall, with the use of endoscopic techniques such as mechanical lithotripsy, electrohydraulic lithotripsy, laser lithotripsy, and ESWL, one report showed successful stone removal in 98% of 217 patients, with only five patients requiring surgery (Schumacher et al, 1998).
Dissolution Therapy
Contact chemical dissolution of stones (see Chapter 28) has been attempted by perfusing the CBD with solvents administered via an indwelling nasobiliary tube, percutaneous transhepatic catheter, cholecystostomy tube, or an existing T-tube. The initial results with these agents were disappointing because of incomplete stone dissolution and complications. A semisynthetic vegetable oil, monooctanoin, composed of 70% glycerol-1-monooctanoate and 30% glycerol-1,2-dioctanoate, was used experimentally for the dissolution of CBD stones beginning in 1977. Results collected from 222 clinicians treating 343 patients with CBD stones between 1977 and 1983 reported a success rate for complete stone dissolution of only 25.6% and an additional partial success rate of 28% (Palmer & Hoffmann, 1986). Serious adverse effects leading to discontinuation of treatment occurred in 5% of patients, including hemorrhage from duodenal ulceration, acute pancreatitis, jaundice, pulmonary edema, acidosis, anaphylaxis, septicemia, and leukopenia, but no deaths were reported. The use of organic solvents, such as the aliphatic ether methyl tert-butyl ether (MTBE) (Allen et al, 1985), also has been disappointing, with complete stone dissolution achieved in only 30% to 45% and an unacceptable complication rate related to systemic absorption from spillover of solvent into the duodenum and intrahepatic bile ducts (Brandon et al, 1988; Diaz et al, 1992; Kaye et al, 1990; Murray et al, 1988; Neoptolemos et al, 1990). Sophisticated computer-controlled two-way pump systems may reduce complications and improve efficacy, but total success for large CBD stones using cholesterol solvents is unlikely, because these stones are composed primarily of bile pigments with small concentrations of cholesterol. Expectations of developing a solvent-chelating agent (ethylenediaminetetraacetic acid) for pigment stones have not been realized. As a result of its low efficacy and morbidity, contact dissolution therapy has not assumed an important role in patients with refractory CBD stones, and newer agents with better methods for instillation are awaited.
Endoprosthesis Placement
In the few situations in which stone extraction is incomplete or impossible because of stone size, local anatomy, bleeding, or technical difficulty leading to incomplete ES, a nasobiliary tube (Fig. 36.9) or endoprosthesis (Fig. 36.10) must be inserted to provide biliary decompression and prevent stone impaction in the distal CBD. This is a temporizing therapy to allow the patient’s clinical condition to improve, until complete stone clearance is achieved via additional endoscopic maneuvers or surgery. In patients with uncertain duct clearance, a follow-up cholangiogram can be obtained via a nasobiliary tube without the need for repeat ERCP.


Nasobiliary tubes are rarely tolerated beyond a few days. The primary problem with tube placement has been accidental dislodgment, and this has led to the alternative therapy of temporary biliary endoprosthesis placement (Kiil et al, 1989; Rustgi & Schapiro, 1991). In a poor-risk surgical patient, ES and long-term placement of a biliary endoprosthesis has been proposed as a nonsurgical alternative (Cotton et al, 1987; Foutch et al, 1989; Nordback, 1989; Soomers et al, 1990). Stent patency is not of major clinical importance in this situation, because the sphincterotomy typically provides an adequate conduit for bile flow around the prosthesis, which then serves principally to prevent stone impaction. The use of oral ursodeoxycholic acid in these patients has resulted in CBD stone disappearance, but additional studies are necessary to determine the true efficacy in this setting (Johnson et al, 1991). Of 84 patients intentionally treated with permanent stents for endoscopically irretrievable stones and followed for a mean of 3 years, 49 (58%) developed biliary complications, and nine died as a result of complications. Most of the patients had a long, symptom-free interval, however, before complications developed, supporting stenting as effective short-term treatment (Bergman et al, 1995; Maxton et al, 1995). In a randomized study with a shorter mean follow-up (1.5 years) that compared placement of a plastic biliary stent with ES as definitive therapy with stone clearance by means of the basket, balloon, or mechanical lithotripter, the patients with stents had a significantly greater rate of cholangitis (36%) than the patients managed by a conventional endoscopic duct clearance approach (14%). The high risk of long-term complications does not support the concept of permanent stent therapy except for patients with severe comorbidity and a short life expectancy.
Results of Endoscopic Therapy
Successful endoscopic treatment of CBD stones requires an adequate ES, which is now achieved in greater than 90% of attempts in most reported series, with noticeable improvement as experience increases (Blumgart & Wood, 1978; Cotton, 1984; Cotton & Vallon, 1981; Geenen et al, 1981; Leese et al, 1985a; Schumacher et al, 1998; Seifert et al, 1982; Siegel, 1981). Although success rates for achieving ES are fairly uniform, rates for complete clearance of the CBD vary because not all endoscopists use extraction methods routinely, and follow-up ERCP may be incomplete. Most experts now would expect to extract stones in at least 90% of successful sphincterotomies. Failure to extract or pass stones may be due to the size or number of stones within the duct or unfavorable duct diameter, usually in its retropancreatic segment. Stones 10 mm in diameter do not give rise to many problems, but in general, with size greater than 15 to 20 mm, the chance of retention increases. Interpretation of success rates necessitates care, because centers with greater expertise are more likely to be referred difficult cases that may be failures from attempts elsewhere, and this would bias some results. Patient groups also vary considerably from unit to unit and country to country, reflecting different referral patterns, selection of patients, and attitudes toward endoscopic therapy. Results from centers around the world (Cotton, 1984; Cotton & Vallon, 1981; Freeman et al, 1996; Geenen et al, 1981; Leese et al, 1985a; Nakajima et al, 1979; Reiter et al, 1978; Safrany, 1978; Schumacher et al, 1998; Seifert et al, 1982; Sherman et al, 1991; Siegel, 1981; Vaira et al, 1989) with individual and collected series of 430 to 9041 patients range from 75% to 96% for duct clearance with a median value of 91%.
Complications of Endoscopic Therapy
Early complications of ES have been well documented, and despite the disparate indications and selection of patients among centers, the incidence seems to be remarkably consistent at 5% to 10% (Cotton, 1984; Cotton & Vallon, 1981; Freeman et al, 1996; Geenen et al, 1981; Leese et al, 1985a; Masci et al, 2001; Seifert et al, 1982; Siegel, 1981; Vandervoort et al, 1996). The expected higher complication rate during early experience with ES is reflected in a single-center series comparing the results of the first 394 procedures (Leese et al, 1985a), which carried an overall morbidity rate of 10.4%, with a subsequent consecutive group of 300 sphincterotomies, in which this rate decreased to less than 6%. However, the respective proportions of individual complications remain similar in most reports: acute hemorrhage from the sphincterotomy site, 2% to 2.9%; acute pancreatitis, 1.5% to 5.4%; cholangitis, 1% to 2.7%; and retroperitoneal perforation, 0.3% to 1%, with small numbers of other problems, such as impacted basket, gallstone ileus, and acute cholecystitis overall accounting for 1.1%. Emergency surgery was required in 1% to 2.5% of cases for bleeding, cholangitis, perforation, and pancreatitis in descending order of frequency. Complication rates must be interpreted with caution, because definitions of hemorrhage, acute pancreatitis, cholangitis, and perforation often differ and are not always given.
A consensus conference provided a set of standards for defining complications and their severity (Cotton et al, 1991a). We have always included any episode of overt bleeding (hematemesis or melena) and a decrease in hemoglobin of 2 g/dL or more after ES as significant hemorrhage, although some authors have included only episodes requiring transfusion. Use of aspirin or related drugs in the usual doses does not seem to increase the incidence of hemorrhage (Freeman et al, 1996). The diagnosis of pancreatitis and cholangitis must depend on the presence of clinically recognizable syndromes rather than asymptomatic hyperamylasemia or transient elevation of temperature alone. There does not seem to be a significant influence on the rate or type of complication based on the initial presentation of the CBD stone (pain alone, jaundice alone, pancreatitis, a combination of these), except that cholangitis and cholecystitis are more likely after ES if cholangitis is preexisting. Present evidence does not suggest that complications are more likely in older patients or after previous biliary surgery (Clarke et al, 2001).
Statistically significant risk factors for complications include difficulty in cannulation, access (precut) papillotomy, suspected sphincter of Oddi dysfunction, more than two pancreatic cannulations, acinarization of the pancreas, failed biliary access or drainage, and technical skill of the endoscopist; the age and general medical condition of the patient were not statistically significant (Freeman et al, 1996; Neoptolemos et al, 1989; Vandervoort et al, 2002). Duodenal diverticula, although sometimes rendering ERCP and ES technically more difficult, do not seem to add any further risk. Many series do not include nonendoscopic complications occurring after ES, such as cardiovascular, cerebrovascular, or respiratory events. In addition, although surgery for the treatment of complications is usually documented, surgery for failed endoscopic therapy is often not documented. These factors are important if comparative data from the surgical literature are to be interpreted correctly.
Management of Complications
The management of complications by centers performing ES is well standardized, but many patients are referred from other hospitals to which they are returned after the procedure, where experience in managing complications may be limited. Of all complications, hemorrhage usually requires surgical intervention, but this occurs only in a few cases. In the rare major arterial hemorrhage, endoscopic view of the papillary area is often obscured completely by blood, and further endoscopic therapy may be impossible. The sphincterotomy usually is converted to a formal surgical sphincteroplasty, which includes the likely bleeding artery. Immediate methods for hemostasis include balloon tamponade, direct bipolar electrocautery, injecting or washing the area with 1 : 10,000 epinephrine solution, application of hemostatic clips, laser coagulation, superselective arterial catheterization and embolization, and infiltration with sclerosant (Grimm & Soehendra, 1983; Leung et al, 1995; Wilcox et al, 2004).
Acute pancreatitis is managed in the standard fashion (see Chapters 53 and 54), and although many attacks are mild and self-limited, clinicians should not be complacent, because some attacks are more severe and should be graded and treated appropriately. Wire-guided cannulation decreases the risk of post-ERCP pancreatitis when compared to the contrast-injection method (Cennamo et al, 2009). There is no evidence that pre-ES or post-ES administration of aprotinin (Trasylol) or glucagon influences the incidence or severity of pancreatitis. In contrast to hemorrhage, the onset of pancreatitis may be delayed for several hours or, rarely, for 1 or 2 days. Gabexate, a synthetic protease inhibitor, and somatostatin have been shown in randomized, double-blind controlled trials to reduce the extent of enzyme elevations and the incidence of pancreatitis after ERCP (Cavallini et al, 1996; Masci et al, 2001; Poon et al, 2003). Gabexate was infused for 30 to 90 minutes before and for 6.5 to 12 hours after ERCP, whereas somatostatin was administered either as a bolus infusion or in a manner similar to gabexate (Bordas et al, 1998; Poon et al, 1999, 2003). A trial suggested diclofenac administered as a rectal suppository after ERCP reduced the incidence of post-ERCP pancreatitis (Murray et al, 2003). Trials using secretin are in progress.
Cholangitis is confined almost completely to patients in whom CBD clearance has not been achieved, and measures should be directed at providing adequate bile drainage (e.g., by nasobiliary catheter or endoprosthesis) and administering parenteral antibiotics (see Chapter 43). Emergency surgery for cholangitis carries high risk but is indicated in patients who do not improve within 24 hours.
Perforation may be asymptomatic and noticed only as retroperitoneal gas (Fig. 36.11) or extravasation of radiographic contrast material, but even in a symptomatic patient, conservative treatment is often effective, with spontaneous resolution and avoidance of potentially difficult surgery. Occasionally, this complication presents late after ES with a retroperitoneal collection of bile or pus in the flank or inguinal region (Neoptolemos et al, 1984a; Leese et al, 1985a) and requires percutaneous or surgical drainage.
Mortality
Death after ES has not been reported in a standardized way. Deaths directly attributable to the procedure are fairly constant at 0.8% to 1.5% (Cotton, 1984; Cotton & Vallon, 1981; Geenen et al, 1981; Leese et al, 1985a; Nakajima et al, 1979; Reiter et al, 1978; Safrany, 1978; Seifert et al, 1982; Siegel, 1981; Sivak, 1989), with almost equal distribution of causes between hemorrhage, pancreatitis, cholangitis, and perforation. Most of the deaths are postprocedural. Mortality rate as a proportion of complications ranges from 7% to 17%, which presumably reflects the comprehensive reporting of all complications by some authors, but reporting of only more severe complications by others. Using the accepted method of reporting 30-day surgical mortality, mortality within 1 month of ES was 3.3% compared with 0.8% immediate postprocedural mortality (Leese et al, 1985a
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


