Chapter 69A Simple cysts and polycystic liver disease
Clinical and radiographic features
Overview
The entity common to simple cysts and polycystic liver disease (PCLD) is a malformation, lined by a nontypical biliary-type epithelium that does not communicate with the biliary tree. This differentiates these diseases from hydatid cysts (see Chapter 68), cystic hepatobiliary neoplasms (Chapter 79B), and cystic dilation of the intrahepatic bile ducts (Chapter 46).
This chapter focuses on pathology, prevalence, manifestation, and diagnosis of PCLD. Differential diagnosis from other cystic lesions is addressed at the end of this chapter, and therapeutic management is addressed in Chapter 69B.
Simple Cysts of the Liver
Pathology and Pathogenesis
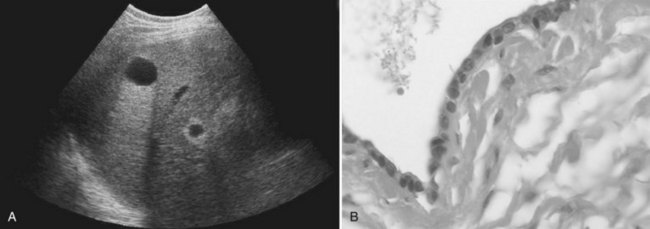
Microscopically, the cysts appear to be bordered by a single layer of cuboid or columnar epithelial cells, resembling biliary epithelial cells (Fig. 69A.1). The cells are uniform, without any atypia. Stroma is absent in small cysts and is reduced to a thin layer of connective tissue in large cysts. Simple cysts of the liver are regarded as a congenital malformation, likely aberrant bile ducts that have lost communication with the biliary tree and dilate progressively. Liver cyst epithelial cells retain differentiated secretory function; they secrete fluid and generate a positive luminal pressure that may be greater than 30 cm H2O, which accounts for most symptoms. The composition of the fluid, which contains water and mineral electrolytes without bile acids and bilirubin, is close to that of the normal secretion of the epithelium of the bile ducts. It is not toxic to the peritoneum, which is the rationale for cyst fenestration (see Chapter 69B).
Prevalence and Etiology
Simple cysts had been considered rare. By 1971, only 350 cases had been reported (Flagg & Robinson, 1967; Moreaux & Bloch, 1971), and early estimates from autopsy studies were less than 1% (Larsen, 1961). However, the development of imaging techniques revealed that simple cysts are much more frequent. Prevalence in ultrasound studies is 3% to 5% (Caremani et al, 1993; Gaines & Sampson, 1989); however, in a more recent spiral computed tomographic (CT) study of an adult population, prevalence was 18% (Carrim & Murchison, 2003). These discrepancies are explained by the usual small size of most cysts, which are discovered only by accurate imaging techniques. An association between simple hepatic cysts and simple renal cysts has been documented (Carrim & Murchison, 2003), but this association has not yet been explained.
The incidence of simple cysts is age and gender related. Simple cysts are uncommonly identified before age 40 years, but their incidence increases sharply thereafter. Simple cysts also are larger in adults older than 50 years (Larsen, 1961). The female/male ratio is 1.5 : 1 for all simple cysts shown at necropsy or imaging; however, this statistic jumps to 9 : 1 in symptomatic or complicated simple cysts (Moreaux & Bloch, 1971). Huge cysts affect women older than 50 years almost exclusively. Based on these observations, the diagnosis of simple cysts should be retained with caution, when a large or symptomatic cystic mass is observed in a male patient or in a young woman.
Manifestations and Diagnosis
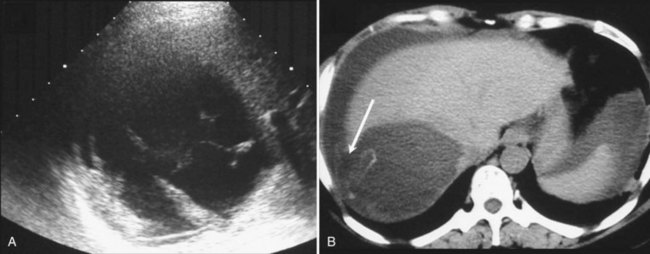
US is the best imaging modality for recognizing simple cysts, which appear as a circular or oval, completely anechoic lesion with sharp, smooth borders and strong posterior wall echoes that indicate a well-defined tissue-fluid interface (Liang et al, 2005). Echoes beyond the cyst are accentuated compared with echoes at a similar depth transmitted through normal adjacent liver tissue (see Fig. 69A.1). Accentuation of the echoes beyond the cyst indicates that the lesion is filled with fluid. This so-called acoustic posterior enhancement is observed only when the deep tissue transmits US; it is not seen when a total reflector, such as gas or bone, lies behind the cyst or when the cyst is very posterior. Neither wall nor septation is apparent, but a false image of septation may be seen when two cysts are adjacent. In some patients, intracystic echoes or material can be detected after intracystic bleeding.
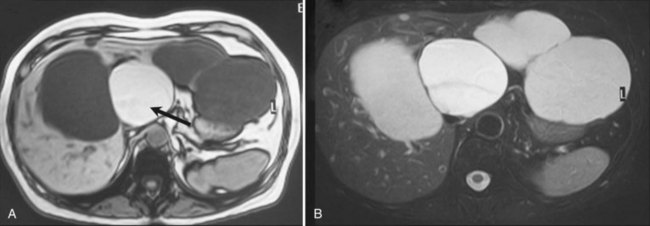
Other imaging procedures have less utility in diagnosis compared with US and are generally not required. CT confirms the presence of one or several round or oval, water-dense lesions but no septations or intracystic formations; dynamic CT shows that such lesions are avascular. In small cysts, recognition of water density may be difficult; the average density of the cyst is obscured by the density of the adjacent liver tissue, but an apparent increase in density may be observed after intravenous injection of contrast medium. On magnetic resonance imaging (MRI), the cyst is homogeneous, very hypointense on T1-weighted images, and very hyperintense on T2-weighted images, as are the gallbladder contents (Fig. 69A.2). If the patient lives or has been living in an area where hydatid disease is endemic, or when any doubt exists about a possible hydatid cyst, serologic tests for this parasitic infection should be performed, although their accuracy is fairly low. MRI should also be performed (see Chapter 68).
Course and Complications
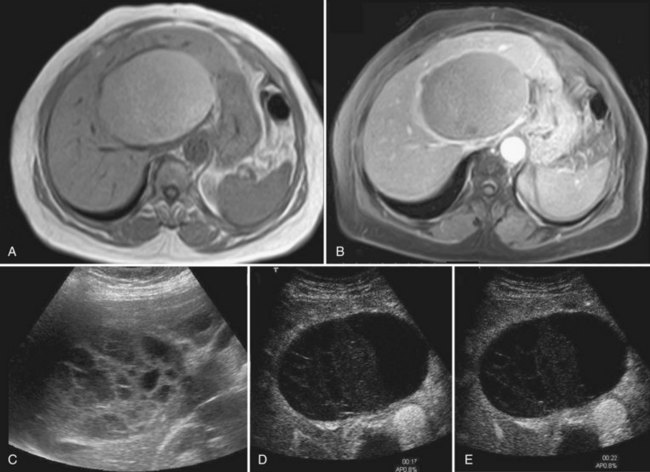
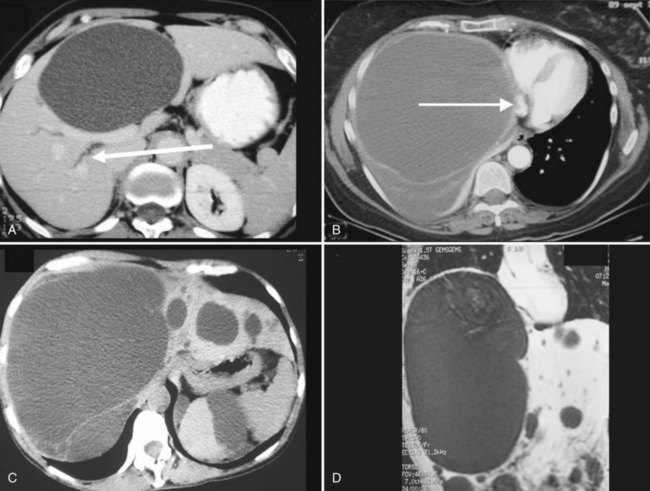
Complications are uncommon, but intracystic bleeding is the most frequent observed (Frisell et al, 1979; Moreaux & Bloch, 1971) and is presumed to result from the erosion of an artery adjacent to the cyst. The clinical manifestations consist of sudden, severe pain and an increase in the size of the cyst. The pain resolves in a few days; in some cases, pain is mild or absent. There is no evidence of anemia, and the biologic liver tests show only a moderate elevation of γ-glutamyltransferase (GGT). On US, echoic material corresponding to clots is seen within the cyst (Fig. 69A.3); this material usually is mobile, sliding in the inferior part of the cyst. Hemorrhagic cysts also become hyperintense on T1-weighted MRI, whereas uncomplicated cysts are hypointense (see Fig. 69A.2). After gadolinium injection, an enhancement of the periphery of the cyst is frequently seen when hemorrhage is recent, which corresponds to compressed liver parenchyma (Fig. 69A.4). Contrast US may also prove useful in the future by showing that neither the cyst wall nor the intracystic material is enhanced, unlike cystadenoma (see Fig. 69A.4; Chapter 79B), but larger studies are required (Akiyama et al, 2008). Communication with the bile duct lumen may develop, presumably also by an erosive mechanism; however, bacterial infection in contrast is exceptional.
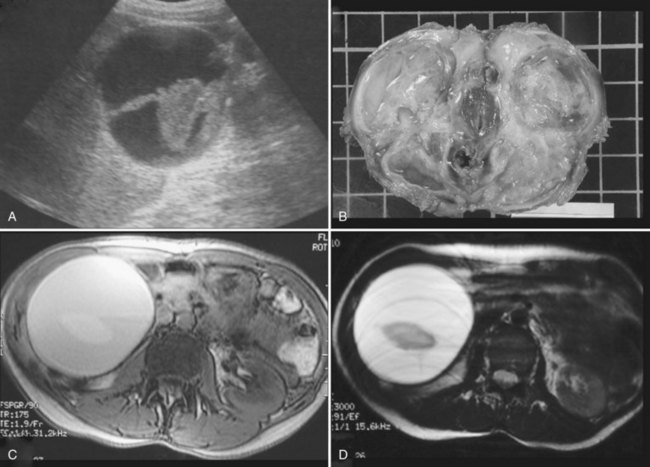
Spontaneous rupture into the peritoneal cavity (Fig. 69A.5; Akriviadis et al, 1989; Salemis et al 2007)—or, more rarely, into the pleural cavity or the duodenum (Williamson et al, 1978)—is exceptional. In contrast to hydatid cysts, peritoneal perforation of simple cysts is self-limited. Severe hemoperitoneum has been described only in patients with PCLD undergoing dialysis.
Because simple cysts are tense, they may compress the bile ducts or the inferior vena cava (Fig. 69A.6), and although anecdotal, there have been reports of pulmonary embolism after clot formation (Buyse et al, 2004). As discussed in Chapter 69B, compression of biliary branches or hepatic veins is a potential source of intraoperative or postoperative complications.
Polycystic Liver Disease
PCLD—or, more precisely, diseases—is a term for genetic disorders responsible for the progressive development of multiple cysts in the liver. PCLD was initially considered to exclusively develop in the context of ADPKD (Moschcowitz, 1906). However, identification of families with PCLD but no ADPKD proved that PCLD may also occur alone (Berrebi et al, 1982; Tahvanainen, et al, 2003). These two forms of PCLD—those with and without ADPKD—are linked to distinct gene mutations. Both, however, have an autosomal dominant transmission and an almost identical clinical course. Of note, one third of patients with isolated PCLD may have a few kidney cysts, usually one or two (van Keimpema et al, 2010), as does the general population of adult patients (Carrim & Murchison, 2003). Distinction between the two forms of PCLD is addressed below.
Genetics
Polycystic Liver Disease and Autosomal Dominant Polycystic Kidney Disease
PCLD associated with ADPKD is linked to mutations in either the PKD1 or PKD2 gene. PKD1 (Ward et al, 1996) is located on the short arm of chromosome 16 and encodes polycystin-1; its mutation accounts for 85% of mutations in ADPKD patients. Most of the rest are related to a mutation in PKD2 (Mochizuki et al, 1996), which is located on chromosome 4 and encodes polycystin-2. PKD1 mutation is associated with more renal cysts, larger cysts, more prevalent hypertension, and faster progression to end-stage renal disease than PKD2 mutation.
Isolated Polycystic Liver Disease
Isolated PCLD—that is, PCLD without ADPKD—is associated with heterozygous mutation in either the Protein Kinase C Substrate 80K-H (PRKCSH) or SEC63 genes. Both genes are located in the endoplasmic reticulum and function in the early secretory route of the cell. PRKCSH is located on the short arm of chromosome 19, which encodes the protein hepatocystin (Drenth et al, 2004). Hepatocystin functions as the β-subunit of α-glucosidase II and is involved in the protein-folding processes and quality control of newly synthesized glycoproteins (Trombetta et al, 2001). SEC63 is located on the long arm of chromosome 6 and encodes the SEC63 protein involved in protein transport across the endoplasmic reticulum membrane (Brodsky et al, 1995). However, these mutations only explain 25% to 40% of cases (Davila et al, 2004; van Keimpema et al, 2010), which suggests that one or more other genes is involved.
The Two-Hit Theory
PCLDs have an autosomal dominant phenotype but are considered to be a recessive disease at the molecular level because they require a second somatic mutation. According to this theory, a germline mutation is present in either PKD1 or PKD2. However, cell proliferation and cyst formation occurs in individual cells that have in addition received a second loss-of-function somatic mutation in the other gene copy (Everson et al, 2004). This second hit would explain why affected cells are few and why cysts develop from place to place; it may also account for the extreme heterogeneity of the disease. This theory has been designed for PCLD associated with ADPKD but has not been investigated for isolated PCLD. It is unclear as to why these various mutations may affect both the liver and kidney or only the liver.
Pathology and Pathogenesis
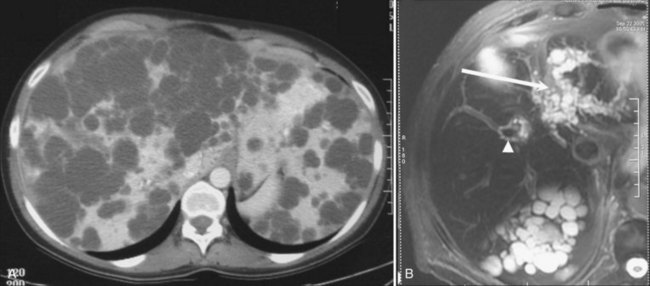
Liver cysts in PCLD are macroscopically and microscopically similar to simple cysts of the liver, and their number and distribution are highly variable. They are lined by a single-layered epithelium that has phenotypic and functional characteristics of biliary epithelium (Perrone et al, 1995) and retain in particular a secretory capacity and responsiveness to secretin (Everson et al, 1990). The cysts result from abnormal remodeling of the ductal plate and mainly arise from dilation of biliary microhamartomas, also known as von Meyenburg complexes, which have lost their communication with the biliary tree (Melnick, 1975). Some cysts also arise from peribiliary glands surrounding large intrahepatic bile ducts (Fig. 69A.7; Kida et al, 1992).
The mechanisms of cyst expansion are still not fully explained but appear similar to those involved in the development of renal cysts. Growth results from a combination of proliferation of epithelial cells, remodeling of the extracellular matrix required for the cyst to invade the surrounding liver parenchyma (Murray et al, 1996), and neovascularization that results in increased density of the vascular bed surrounding the cysts (Bello-Reuss et al, 2001; Nichols et al, 2004).
As in the kidney tubules, the microvilli and long cilia normally on cholangiocytes are believed to play a dominant role. These mechanosensory organelles may be bent by bile flow and can also react to hormonal, morphogen, or growth factor stimuli; they may even function as sensors of cell injury. These cilia and microvilli modulate concentrations of intracellular levels of cyclic adenosine monophosphate (cAMP) and Ca2+ that are mediators of proliferation and secretory activity of cholangiocytes. In PCLD, these cilia progressively disappear from the luminal surface of the epithelium as cysts enlarge (Alvaro et al, 2008). Their absence could impair Ca2+-dependent counterregulation of cAMP, which is a key determinant of cholangiocyte proliferation. It is unclear whether the disappearance of these cilia is a primary event or a result of increased pressure. However, polycystin-1 and polycystin-2 are localized to the cilia, and their absence as a result of a PKD1 or a PKD2 mutation could result in ciliary dysfunction. In patients with isolated PCLD, it has been postulated that polycystins could be the target of aberrant maturation of newly synthesized glycoprotein caused by PRKCSH or SEC63 mutations.
Two other targets of the cell cycle have been identified. One is the mammalian target of the rapamycin (mTOR)-mediated signaling cascade (Shillingford et al, 2006), which explains growing interest from the industry for mTOR inhibitors (see Chapter 69B). The other is through micro-RNAs, small, noncoding RNAs that inhibit target messenger RNA transcripts via sequence-specific base paring; micro-RNA-15a in particular is downregulated in cyst epithelium, resulting in an overexpression of Cdc25A, which activates cyclin-dependent kinases and progression of the cell cycle (Lee et al, 2008).
Fluid secretion by the epithelium lining the cyst may also contribute to cyst expansion. Ciliary dysfunction could also play a role because it has also been shown to result in maintenance of an immature phenotype by biliary epithelial cells with postnatal expression of developmental proteins. A variety of cytokines and growth factors present in increased concentration in the cysts have been implicated in cyst growth by autocrine-paracrine signaling (Alvaro et al, 2008; Fabris et al, 2006; Nichols et al, 2004). Angiogenic factors in particular could play a role by promoting vascularization of the cyst and also by directly stimulating cholangiocytes. Furthermore, the epithelium stains positive for insulin growth factor 1 (IGF-1) and its receptor, as well as for estrogen receptors (Alvaro et al, 2008), and is particularly sensitive to this signaling.
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Bile duct exploration and biliary-enteric anastomosis
Bile duct exploration and biliary-enteric anastomosis
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


