Fig. 17.1
Gram-negative intracellular diplococcus
Peak incidence for all forms of gonorrhea is in the late teens for females and early 20s for males. African Americans have a 30-fold higher rate of infection than do White Americans.
Infection from N. gonorrhoeae occurs in columnar, cuboidal, or noncornified epithelial lined cells of the urethra, endocervix, rectum, and pharynx and is frequently asymptomatic. The incubation period ranges from 3 days to 2 weeks.
Untreated infection may lead to disseminated gonococcal infection with transient bacteremia, arthritis, and dermatitis. Rare but severe sequelae include endocarditis and meningitis.
Anorectal transmission in homosexual males and in some females is by anoreceptive intercourse with an infected partner.
Thirty-five to fifty percent of women with gonococcal cervicitis have concomitant rectal infection, which is believed to be from contiguous spread from the genital infection.
A large percentage of patients who culture positive for rectal gonorrhea are asymptomatic – up to 50 % of males and 95 % of females. Asymptomatic rectal infection constitutes the main reservoir of gonococcal disease in homosexual men.
Symptomatic anorectal gonococcal infection results in pruritus, tenesmus, bloody discharge, mucopurulent discharge, or severe pain (Fig. 17.2).

Fig. 17.2
Anorectal gonorrhea
Anoscopy reveals a thick purulent discharge, which classically is expressed from the anal crypts as pressure is applied externally on the anus. Nonspecific proctitis may be present with erythema, edema, friability, and pus.
Diagnosis is confirmed by culture on selective media (Thayer–Martin or Modified New York City) incubated in a CO2-rich environment and Gram stain of directly visualized discharge. The use of lubricants other than water may introduce antibacterial agents during anoscopy and decrease diagnostic yield.
Nonculture detection of gonorrhea is being used more frequently especially in urethral and cervical infections but is not currently licensed for the detection of rectal gonorrhea.
The most current recommended treatment regimen from the Centers for Disease Control (CDC) is listed in Table 17.1. Concurrent HIV infection does not alter treatment for anorectal gonorrhea. Because of the high rate of concomitant infection with chlamydia, patients treated for gonococcal infections should be given appropriate treatment for Chlamydia at the same visit or measures to exclude chlamydial infection should be taken.
Table 17.1
Treatment of anorectal gonococcal infection
One of the following as a single dose |
Ceftriaxone – 125 mg IM |
Ciprofloxacin – 500 mg orally |
Ofloxacin – 400 mg orally |
Levofloxacin – 250 mg orally |
Cefixime – 400 mg orally |
Routine follow-up at 3 months is no longer necessary since current treatment provides near 100 % efficacy.
Patients with persistent symptoms after treatment should be followed and cultured as should those treated with nonstandard antibiotics.
Sexual partners from the past 60 days should be treated, and patient should abstain from intercourse until treatment is completed and symptoms resolved.
Chlamydia/Lymphogranuloma Venereum (LGV)
Chlamydia trachomatis is an obligate intracellular bacterium that is sexually transmitted and results in clinical infections that are similar to those caused by N. gonorrhoeae.
Simultaneous infection with both organisms is common.
Chlamydia is the most commonly reported STD in the USA with an annual incidence of about three million cases per year.
Anorectal transmission of chlamydia is through anoreceptive intercourse although secondary involvement can occur as a late manifestation of genital infection.
Different serovars of C. trachomatis produce differing clinical illness. Serovars D through K (non-LGV) are responsible for proctitis and common genital infections.
Lymphogranuloma venereum is caused by LGV serovars L1–L3. The incubation period for Chlamydia is 5 days to 2 weeks.
Non-LGV serovars are less invasive and cause mild proctitis (manifest by tenesmus, pain, and discharge), but asymptomatic infection is common.
LGV serovars produce a much more aggressive infection with perianal, anal, and rectal ulceration. The proctitis produced can be difficult to distinguish from Crohn’s disease (including microscopic findings of granulomas) with resulting rectal pain and discharge.
Anoscopy and sigmoidoscopy demonstrate friable rectal mucosa, which is more severe in appearance (and extends above the rectum in some cases) in LGV strains. Perianal abscesses, fistulas, and strictures may also occur. Lymphadenopathy develops in draining nodal basins, including the iliac, perirectal, inguinal, and femoral regions, several weeks after initial infection. Large indurated matted nodes and overlying erythema may produce a clinical picture similar to syphilis (Fig. 17.3).

Fig. 17.3
Inguinal adenopathy of LGV; LGV lymphogranuloma venereum
Diagnosis of chlamydia as the causative agent in proctitis can be difficult.
Proper specimen collection increases diagnostic yield and consists of a cotton or Dacron swab with an inert shaft (plastic or metal). Specimen for tissue culture should be transported on specific medium and kept refrigerated or on ice until inoculated onto culture plates. Specimens that are to be tested by a nonculture technique are transported and stored in accordance with the test manufacturers guidelines. In patients with a clinical presentation consistent with chlamydia proctitis, rectal Gram stain showing polymorphonuclear leukocytes without visible gonococci is presumptive for a diagnosis of chlamydia.
Tissue culture for chlamydia is relatively insensitive and is not widely available because of cost and technical requirements.
Antigen detection by direct fluorescent antibody (DFA) or enzyme immunoassay DFA is highly specific, widely available, and does not require rapid transportation or refrigeration. A trained microscopist is needed for interpretation.
The two recommended treatment regimens for rectal chlamydia (non-LGV) are azithromycin, 1 g orally as a single dose or doxycycline, 100 mg orally, twice a day for 7 days. Management of sexual contacts is the same as for gonorrhea. Abstinence from sexual intercourse should last until 7 days after treatment with azithromycin or completion of 7 days of doxycycline.
Syphilis
Syphilis is an STD caused by the spirochete Treponema pallidum that can present in one of several progressive stages – primary (chancre or proctitis), secondary (condyloma lata), or tertiary.
The primary stage of anorectal syphilis appears within 2–10 weeks of exposure via anal intercourse. The chancre begins as a small papule that eventually ulcerates. Anal ulcers are frequently painful (in contrast to genital ulcers) and without exudates. They may be single or multiple (Figs. 17.4 and 17.5) and located on the perianal skin, in the anal canal or distal rectum. Differentiation from idiopathic anal fissures may be difficult. Painless but prominent lymphadenopathy is common. Proctitis from syphilis may occur with or without chancres. Untreated lesions in this stage usually heal in several weeks.

Fig. 17.4
Solitary anal chancre

Fig. 17.5
Multiple anal chancres
Hematogenous dissemination of untreated syphilis leads to a secondary stage that occurs 4–10 weeks after primary lesions appear. Nonspecific systemic symptoms from this infection include fever, malaise, arthralgias, weight loss, sore throat, and headache. A maculopapular rash is seen on the trunk and extremities. Condyloma lata, another secondary manifestation, are gray or whitish, wartlike lesions that appear adjacent to the primary chancre and are laden with spirochetes.
Untreated, the symptoms of syphilis usually resolve after 3–12 weeks – of these patients, approximately one-fourth have a relapse of symptoms in the first year, a stage known as early latent syphilis.
Diagnosis in the primary or secondary stage is made by visualization of spirochetes on dark-field microscopic exam of scrapings from chancres (Fig. 17.6).
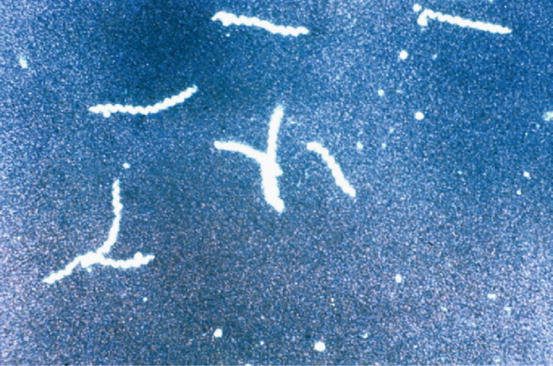
Fig. 17.6
Spirochetes demonstrated on dark-field microscopy
A single intramuscular injection of 2.4 million units of benzathine penicillin G is the treatment for primary and secondary syphilis. Penicillin-allergic patients are treated with doxycycline (100 mg orally, twice daily for 14 days) or tetracycline (500 mg orally, four times a day for 14 days). Follow-up serology (VDRL or RPR) should be checked at 6 months after therapy for HIV-negative patients and every 3 months for HIV-positive patients.
Partner notification, testing, and treatment depend on stage at diagnosis of the index case. At-risk partners include sexual contacts (a) within the prior 3 months plus duration of symptoms for patients with primary syphilis, (b) within the prior 6 months plus duration of symptoms for patients with secondary syphilis, and (c) within the prior year for those with early latent syphilis.
Chancroid
Chancroid is an ulcerating STD caused by the Gram-negative, facultative anaerobic bacillus Haemophilus ducreyi.
Transmission of H. ducreyi is strictly via sexual contacts through breaks in the skin during intercourse and results in genital ulcers.
The initial manifestation (hour to days after exposure) is an infected tender papules with erythema that subsequently develop into pustules and then (days to weeks) become ulcerated and eroded. Multiple ulcers are common and are generally painful, especially in males.
Painful inguinal adenopathy accompanies half of cases in males and is usually unilateral. Females are less likely to develop adenopathy from H. ducreyi infection.
Abscess formation may result, necessitating drainage.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree






