Chapter 92 Segment-oriented anatomic liver resections
Overview
Decreased intraoperative blood loss and preservation of parenchyma are key contributors in recent advances in liver surgery that have resulted in reduced morbidity and mortality in liver resection. The understanding of the segmental anatomy of the liver has been pivotal in the evolution of a safe liver surgery (Scheele et al, 1995). Segmental liver resection offers maximum preservation of liver parenchyma with minimal blood loss and without compromising oncologic safety (Agrawal & Belghiti, 2011; Billingsley et al, 1998; Bismuth et al, 1988; Machado et al, 2003; Polk et al, 1995). The ability to resect one or more segments, rather than the entire lobe, allows parenchymal preservation in patients with diseased parenchyma or in re-resection patients with limited residual volume. Segmental vascular inflow control facilitates the resection by precisely mapping the transection plane. In addition, anatomic resections that involve the removal of a hepatic segment confined by tumor-bearing portal tributaries for the eradication of intrahepatic metastases in the vicinity of the primary tumor represent an oncologic approach to liver resection for some malignant tumors (Agrawal & Belghiti, 2011; Liau et al, 2004).
Anatomy and Terminology
The current understanding of the segmental anatomy of the liver has come from the original 1952 descriptions of Claude Couinaud (1952a, 1952b, 1956). Based on his analysis of vascular and biliary casts of the liver, Couinaud determined that the human liver consists of eight segments, each with its own portal triad—vein, hepatic artery, and hepatic duct—and hepatic venous outflow. Subsequently it has been shown that each segment can be resected independently (Bismuth et al, 1982). These segments have evolved to become the standard for hepatic nomenclature. This so-called Brisbane terminology (Pang, 2002) eliminates confusing lobes and sectors used in the American, European, and Japanese descriptions of liver anatomy. The terms hemiliver (first-order division), section (second-order division), and segment (third-order division) are not interchangeable; these provide universal terminology for better communication among liver surgeons.
The first-order divisions are right liver (segments V through VIII) and left liver (segments I through IV), or hemiliver, the boundary of which lies along the Cantlie line marked by the path of the middle hepatic vein (MHV), from the middle of the gallbladder fossa to its termination in the inferior vena cava (IVC) (Fig. 92.1). The second-order division into liver sections is based upon hepatic arterial supply and biliary drainage. The sections are derived from the primary divisions of the major right and left portal triads. The right hemiliver is divided into sections known as the right anterior (segments V and VIII) and right posterior (segments VI and VII), separated by the right hepatic vein (RHV). The left hemiliver is divided into left lateral (segments II and III) and left medial (segments IVa and IVb) sections by the umbilical fissure and falciform ligament. Together segments II and III are often erroneously referred to as the left lateral segment.
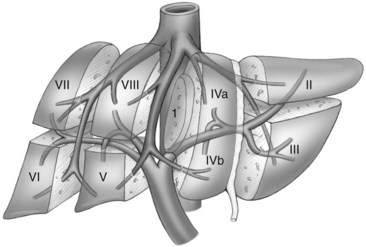
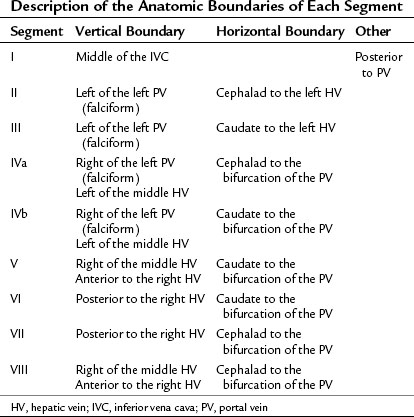
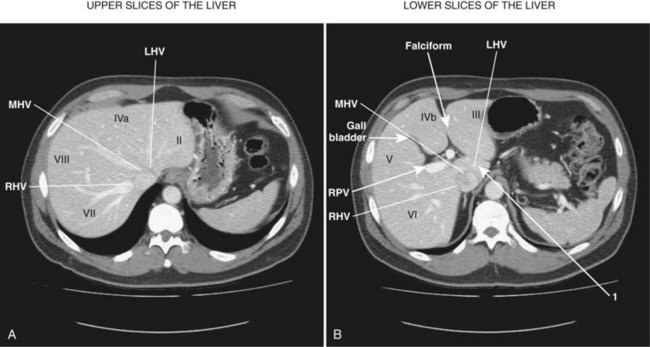
The third-order division, segments I through VIII, is defined by hepatic arterial supply and biliary drainage. The axial plane is at the level of the intersection of the hepatic veins and the axial plane of the bifurcation of the portal vein (Table 92.1 and Fig. 92.2). When considering a segmental resection, it is important to identify the common anomalies that may determine resectability. The biliary and arterial anomalies are the most common: about 30% of patients have a major arterial anomaly, and up to 50% have nonstandard biliary anatomy.
Patient Selection
A liver resection based on the segmental anatomy should be the first consideration for any liver resection. Excluding the fenestration of liver cysts or small “wedge excisions” of superficial lesions, an understanding of the patient’s segmental liver anatomy is essential to a safe, controlled resection. This technique is applicable for all types of livers and indications for resection (Hasegawa et al, 2005).
Achieving balance between parenchymal sparing and radical oncologic clearance is of the utmost importance in hepatocellular carcinoma (HCC) patients with cirrhosis. Segmental liver resection forms a bridge between major hepatectomy and nonanatomic resection to preserve maximum liver volume and prevent postoperative liver failure (Agrawal & Belghiti, 2011; Wakai et al, 2007). Replacement with nonanatomic resection should be done only when the anatomy is unsuitable, or when the residual liver would be at high risk for complications. Segmental liver resection is preferred in patients who have colorectal metastasis with multifocal lesions and are undergoing preoperative chemotherapy, which is frequently associated with steatosis and hepatic cirrhosis (DeMatteo et al, 2000).
General Operative Principles
Preoperative Assessment and Anesthesia
The preoperative assessment and preparation of the patient for a liver resection have been described in Chapter 2. Comorbidities should be identified and optimized. Careful assessment of liver function is important, particularly in those with intrinsic liver disease. Preoperative decompression of an obstructed biliary tree should be considered for improving postoperative liver function (Belghiti & Ogata, 2005). Volumetric analysis should be performed in patients with potentially marginal residual liver size and function. Preoperative portal vein embolization (PVE) may facilitate the safety of a complex or extended liver resection by inducing regeneration of the potential contralateral remnant liver segments (Abulkhir et al, 2008). Particular attention should be paid to the reduction of the central venous pressure during transection to reduce blood loss, and measures to prevent hypothermia are also important. The appropriate prophylaxis of infections and venous thromboembolism is required.
Intraoperative Assessment
Intraoperative assessment of the liver requires correlation of the findings of inspection and palpation of the mobilized liver with those of the preoperative imaging. Intraoperative US has been advocated to localize the lesion and further stage the proposed remnant liver (Makuuchi et al, 1991); however, with the increased precision of preoperative imaging, intraoperative ultrasound (IOUS) seldom alters the procedure (Jarnagin et al, 2001). IOUS of the liver may be valuable to identify venous tumor thrombus and to assess the proposed plane of transection and its relationship with major hepatic veins and portal triads.
Recently, systematic segmentectomy and subsegmentectomy by IOUS-guided finger compression has been described (Torzilli et al, 2010). This technique can be applied in each segment of liver, as long as the thickness of the parenchyma and the anatomy of liver are suitable. IOUS-guided finger compression of the vascular pedicle feeding the tumor at the level closest to it results in a demarcation area, allowing oncologic resection.
Transection Techniques
There are at least two distinct philosophies of liver transection, which result in distinct surgical techniques and surgical styles. The first is that blood loss from the transected liver is minimized by speed, external compression, vascular occlusion (outflow and/or inflow) (Bismuth et al, 1989; Stephen et al, 1996), and the use of surgical interventions to stop bleeding using cautery, sutures, and tissue glues. The second is that blood loss is best minimized by prevention of injury to vascular structures, using transection techniques that dissect out structures from the surrounding parenchyma as understood and anticipated by preoperative imaging and planning. Use of the Cavitron Ultrasonic Surgical Aspirator (CUSA; Valleylab, Boulder, CO), which reduces blood loss better than the clamp-crushing technique (Fan et al, 1996), has become the standard technique of liver transection even in cirrhotic liver (Takayama et al, 2001).
More recently, a third technique has been described that reflects a philosophy of prevention of bleeding that uses destructive hemostatic control of the parenchyma before transection (Ayav et al, 2007; Curro et al, 2008). We prefer the second approach, although clamp crushing, the conventional method of liver transection, is still used in some centers (Imamura et al, 2003; Jarnagin et al, 2002; Lin, 1974). Surgical techniques that facilitate a precise, controlled transection of liver parenchyma and allow the dissection of intrahepatic structures are the Helix Hydro-Jet dissector (ERBE USA, Marietta, GA) (Baer et al, 1991) and the CUSA dissector (Little & Hollands, 1991). Each provides selective destruction of liver parenchyma with relative sparing of denser fibrotic tissue, such as hepatic veins and portal triads. Inflow and outflow vascular occlusion may be added to these techniques for better hemostasis. Because no evidence clearly supports the superiority of any one technique (Clavien et al, 2003), the transection method for any particular operation should be dependent on local expertise.
Techniques that achieve destructive control of the parenchyma and any crossing structures before division include linear cutting staplers, in-line radiofrequency ablation (Habib; Angiodynamics, Latham, NY), and bipolar cautery (Gyrus, Gyrus ACMI, Southborough, MA; and LigaSure, Covidien, Boulder, CO). In-line radiofrequency ablation (RFA) allows surgeons to perform minor and major hepatectomies with minimal blood loss, low blood transfusion requirement, and reduced mortality and morbidity (Ayav et al, 2008); however, this device is seldom used in tertiary reference centers because of concerns about the preservation of venous drainage of the remnant liver and the risk of postoperative bile leak and necrosis (Kim et al, 2003; Lupo et al, 2007). The role of this technology is probably limited to segmental or wedge excision because of the potential risk of bile duct injury, when using this instrument near the liver hilum, and its inability to control bleeding from large venous branches.
Pretransection vascular control is used by many surgeons with oncologic, anatomic delimitation and hemostasis (Bismuth et al, 1989; Stephen et al, 1996
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


