■ Alternatively, the patient can be placed in the low lithotomy position to avoid instrument conflict with the lower extremities. The knees should be slightly flexed and the feet firmly planted on the stirrups to prevent undue pressure on the calves and on the lateral peroneal nerves.
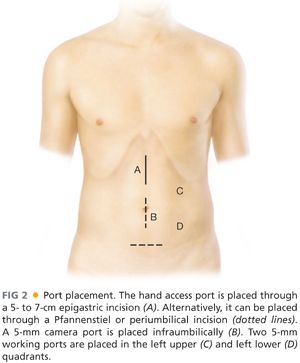
■ Depending on the location of pathology and body habitus, a 5- to 7-cm incision is made for the hand port in an epigastric, periumbilical, or Pfannenstiel location (FIG 2).
■ Location of the trocars can be variable based on surgeon’s preference. In general, it is best to triangulate all ports to enhance visualization and to prevent instrument conflict inside the abdomen.
■ A traditional port placement includes (FIG 2)
■ A GelPort hand port through a 6-cm epigastric incision
■ A 5-mm infraumbilical camera port
■ A 5-mm left lower quadrant instrument port
■ A 5-mm left upper quadrant/left anterior flank
TECHNIQUES
EXPOSURE
■ After placement of the hand port, the abdomen is explored to locate the lesion, to assess the extent of spread, and to palpate the liver and peritoneal cavity for distant metastatic spread.
■ In female patients, the ovaries should be examined for metastatic spread or primary neoplasms.
■ Pneumoperitoneum is created with carbon dioxide (CO2) and additional trocars are inserted.
■ Patient is placed in a left lateral tilt and slight Trendelenburg position. The small bowel is fanned out along its mesentery to aid in the exposure of the right colon.
■ The greater omentum along with the transverse colon is retracted cephalad.
■ The cecum is grasped with the hand and retracted toward the anterior abdominal wall using gentle traction to identify the ileocolic vessels.
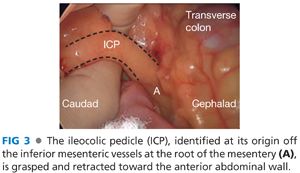
■ The ileocolic pedicle is grasped and retracted toward the anterior abdominal wall (FIG 3).
DIVISION OF ILEOCOLIC PEDICLE
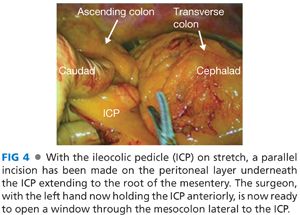
■ With the ileocolic pedicle on stretch, a parallel incision is made on the peritoneal layer underneath the pedicle (FIG 4) extending to the root of the mesentery and the superior mesenteric vein, using monopolar electrocautery.
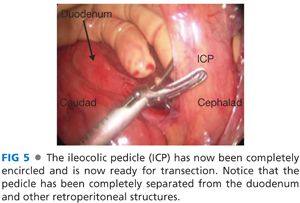
■ A window is created under the ileocolic pedicle in the avascular plane that separates the pedicle from the retroperitoneum (FIG 5).
■ The ileocolic pedicle is isolated and divided close to its origin off the superior mesenteric vessels using an energy device, a linear vascular stapler, or surgical clips based on surgeon’s preference (FIG 6).

MOBILIZATION OF RIGHT MESOCOLON
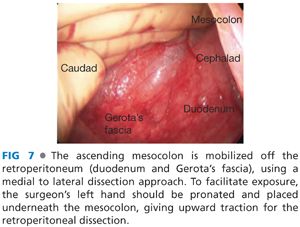
■ Using blunt dissection with a 5-mm energy device, the ascending mesocolon is mobilized off the retroperitoneum (duodenum and Gerota’s fascia) using a medial to lateral dissection approach.
■ To facilitate exposure, the surgeon’s left hand should be pronated and placed underneath the mesocolon, giving upward traction for the retroperitoneal dissection (FIG 7).
■ Mobilization of the right mesocolon is carried out laterally to the abdominal wall (FIG 8A), superiorly to the hepatorenal recess (FIG 8B), and medially exposing the third portion of the duodenum (FIG 8C).

■
Related posts:
 End and Diverting Loop Ileostomies: Creation and Reversal
End and Diverting Loop Ileostomies: Creation and Reversal
 Parastomal Hernia
Parastomal Hernia
 Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
 Right Hemicolectomy: Open Technique
Right Hemicolectomy: Open Technique
 Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
 Total Abdominal Colectomy: Laparoscopic Technique
Total Abdominal Colectomy: Laparoscopic Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


