Fig. 26.1
Patient and team positioning
26.2.2 RPLS
A 3.5 cm transverse skin incision is made in the midline, 1 cm above the pubic symphysis (Fig. 26.2). The underlying fascia is divided in a transverse fashion for 1.5 cm, which expose the rectus abdominis muscle. Anterior and posterior flaps are developed in the avascular plane separating the fascia from the underlying muscle. A purse-string suture using PDS 1 is placed in the fascia. The peritoneum is entered through the midline with a 1 cm incision, and a new purse-string suture using Vicryl 1 is placed. An 11-mm reusable metallic (or a 12-mm disposable) trocar is inserted into both purse-string sutures in order to accomodate a 10-mm, 30° rigid and standard length scope (Karl Storz-Endoskope), and the pneumoperitoneum is created. Two 6-mm reusable flexible trocars (Karl Storz-Endoskope) are inserted at 3 and 9 o’clock position in the respect of the patient head, outside the purse-string sutures (Fig. 26.3). Curved reusable instruments according to DAPRI (Karl Storz-Endoskope) are inserted through the 6-mm flexible trocars (Fig. 26.4a–h). The flexible trocar located at 9 o’clock position accomodates only one instrument, which is the bicurved grasping forceps I (Fig. 26.4a), and the flexible trocar located at 3 o’clock position accomodates the other tools like the monocurved grasping forceps IV (Fig. 26.4b), the monocurved coagulating hook (Fig. 26.4c), the monocurved bipolar grasping forceps and scissors (Fig. 26.4d, e), the monocurved dissecting forceps (Fig. 26.4f), the monocurved scissors (Fig. 26.4g), the monocurved needle holder I (Fig. 26.4h), the monocurved suction and irrigation cannula, and the straight 5-mm clip applier (Weck Hem-o-lok, Teleflex Medical, Brussels, Belgium).
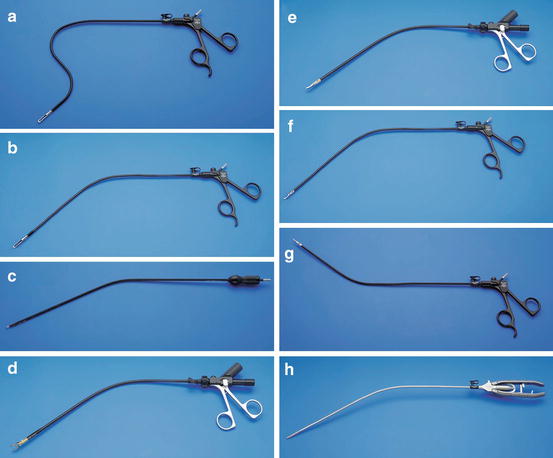
Fig. 26.2
Suprapubic access: a 3.5 cm transverse skin incision is made in the midline, 1 cm above the pubic symphysis
Fig. 26.3
Suprapubic access: insertion of an 11-mm reusable metallic and two 6-mm reusable flexible trocars (Karl Storz-Endoskope)
Fig. 26.4
Curved reusable instruments according to DAPRI (Karl Storz-Endoskope): bicurved grasping forceps I (a), monocurved grasping forceps IV (b), monocurved coagulating hook (c), monocurved bipolar grasping forceps (d), monocurved bipolar scissors (e), monocurved dissecting forceps (f), monocurved scissors (g), monocurved needle holder I (h)
During this procedure if an assistant grasper is necessary, a needlescopic grasper, or the DAPRI 1.8-mm trocarless grasping forceps (Karl Storz-Endoskope) (Fig. 26.5), or a classic 5-mm instrument, is inserted in the left hypocondrium under the rib.
Fig. 26.5
1.8-mm trocarless grasping forceps according to DAPRI (Karl Storz-Endoskope)
The abdominal cavity is explorated to rule out the presence of peritoneal metastases, superficial hepatic lesions and free peritoneal fluid.
The operative table is initially placed in a moderate Trendelenburg position with left-sided tilt. The transverse colon is exposed by reflecting the greater omentum, and the small bowel is gently swept out of the right quadrants of the abdomen, until the last bowel loop is identified. This loop is grasped by the bicurved grasping forceps I, and the mesentery is separated from the peritoneal sheet using the monocurved coagulating hook (Fig. 26.6a, b). The terminal ileum, cecum and the ascending colon are freed from the subperitoneal fascia. The right mesocolon is also mobilized and the right mesocolon is dissected using a lateral-to-medial approach. This dissection is carried superiorly, respecting Gerota’s fascia, until the second and the third portion of the duodenum are idientified (Fig. 26.7a, b). An internal working triangulation as well as an external surgeon’s ergonomy like in multiport laparoscopy is established thanks to the curves of the instruments.
Fig. 26.6
Lateral-to-medial approach: incision of the mesentery of the last bowel loop and separation from the parietal peritoneal sheet using the monocurved coagulating hook (a), under ergonomic surgeon’s conditions (b)
Fig. 26.7
Lateral-to-medial approach: mobilization of the ileo-caecal valve and of the right mesocolon from the parietal peritoneal sheet (a), under ergonomic surgeon’s conditions (b)
For the mesocolon mobilization, the operative table is positioned without any Trendelenburg and tilt. By grasping the mesentery and the right mesocolon with the bicurved grasping forceps I, sufficient tension is applied for section, using the monocurved coagulating hook or the monocurved bipolar scissors and forceps, respecting the medial limit of the superior mesenteric vein (Fig. 26.8a). The surgeon is able to work without crossing hands or clashing instruments’ tips and with an optimal triangulation (Fig. 26.8b). The ileo-cecal vessels, the right colic vessels, and the right branch of the middle colic vessels are exposed at their root and dissected using the monocurved dissecting forceps. These vessels are individually clipped at their root using a 5-mm straight clip applier (Fig. 26.9a, b), and divided with the monocurved scissors (Fig. 26.10a, b).