Chapter 93B Preoperative portal vein embolization
Technique
Overview
Portal vein embolization (PVE) is performed preoperatively to reduce the risk of extensive surgery in patients with small anticipated remnant livers (Makuuchi et al, 1990; de Baere et al, 1993; Abdalla et al, 2002; Madoff et al, 2005a; see Chapter 30a). PVE redirects portal blood flow to the intended future liver remnant (FLR) in an attempt to initiate hypertrophy of the nonembolized segments, and it has been shown to improve the functional reserve of the FLR before surgery. In appropriately selected patients, PVE has also been shown to reduce perioperative morbidity, and it allows for safe, potentially curative hepatectomy for patients previously considered ineligible for resection based on anticipated small remnant livers (Azoulay et al, 2000; Madoff et al, 2005a; Abulkhir et al, 2008). For this reason, PVE is now performed at many comprehensive hepatobiliary centers worldwide prior to major hepatectomy. This section details the techniques currently used to perform PVE, discusses their advantages and disadvantages, and reviews the potential complications that can occur from this procedure.
Technical Aspects of Portal Vein Embolization
Access Routes to the Portal Venous System
PVE can be performed by any of three standard approaches: 1) the intraoperative transileocolic venous approach, 2) the transhepatic contralateral approach (i.e., percutaneous portal vein is accessed via the FLR), and 3) the transhepatic ipsilateral approach (i.e., percutaneous portal access is via the liver to be resected; Madoff et al, 2005a). It is important to note that the approach to the portal vein is chosen at the discretion of the operator, and the decision may be based on multiple factors, including the extent of the embolization and surgery, the operator’s preference for a specific embolic agent, tumor burden within the liver, and the operator’s level of experience with one technique over another (Avritscher et al, 2008). An alternative approach, portal vein ligation, is typically performed intraoperatively during the first stage of a two-stage resection for hepatic colorectal metastases, and it has been reported to be as effective as percutaneous embolization methods (Aussilhou et al, 2008). Regardless of the technique used, the operator must be aware of variations in portal venous anatomy that may impact the conduct of the procedure (see Chapter 1B).
Transileocolic Venous Approach
The transileocolic venous approach was the first approach described for performing preoperative PVE, and it is still used in many Asian centers. This technique is performed at laparotomy by direct cannulation of the ileocolic vein and introduction of a catheter into the portal system for embolization (Abdalla et al, 2002). Conventional teaching has been that this approach is performed when additional treatment is needed during the same surgical exploration, when a percutaneous approach is not considered feasible, or when an interventional radiology suite is not available (Azoulay et al, 1995; Denys et al, 2002).
Percutaneous Transhepatic Ipsilateral Approach
The percutaneous transhepatic ipsilateral approach was first described by Nagino and coworkers (1996), and it is now advocated by many other investigators (Madoff et al, 2003, 2005b; Gibo et al, 2007; Tsuda et al, 2006). With this approach, access is obtained through the portal branches within the tumor-bearing liver (Fig. 93B.1). A distinct advantage of the ipsilateral approach is that the FLR is not instrumented. It also allows for straightforward catheterization of segment IV branches, should embolization of segment IV be required. When planning the puncture, the anterior segment of the right portal vein is preferred, because its use is associated with a lower complication rate (Kodama et al, 2002); however, catheterizing the right portal branches can be challenging, owing to the sharp angulation of the right portal veins, which often necessitates using reverse-curve catheters or balloon occlusion catheters with multiple lumina (Nagino et al, 1996, 2000a).
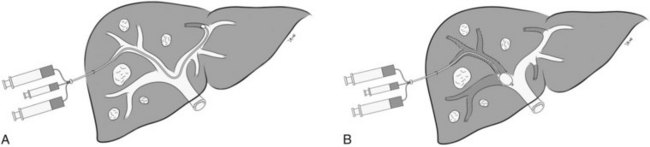
In Nagino’s approach (see Fig. 93B.1), the right anterior portal vein is punctured using sonographic guidance, and a 6-Fr sheath is introduced into the right portal vein system (Nagino et al, 2000a). To make this procedure feasible, the authors designed two types of 5.5-Fr triple-lumen balloon catheters. The first catheter, “type 1,” was designed with one lumen connected to the balloon and two lumina connected to the tip. The second catheter, “type 2,” had two separate lumina opening proximal to the balloon, and the balloons were used to prevent any backflow of embolic material. Both catheters had two separate lumina so that fibrin glue and iodized oil could be injected simultaneously. To facilitate resection, the authors advocated that a proximal right portal vein segment at least 1 cm in length remain patent. Depending on the portal vein anatomy, and the need to spare the proximal right portal vein, type 1 or type 2 catheters were used for embolization. The type 1 catheter was used for embolization of branches distal to the catheter tip, whereas the type 2 catheter was used for embolization of branches proximal to the catheter tip, as mandated by each patient’s portal vein anatomy.
In a recent study, Gibo and coworkers (2007) reported on a modified technique utilizing a four-lumen balloon catheter in eight patients. The authors recommended using this modified catheter because of its larger occlusion balloon and lumina, which allow for safer and easier embolization using fibrin glue. Unfortunately, neither the original nor the modified catheters are available in the United States.
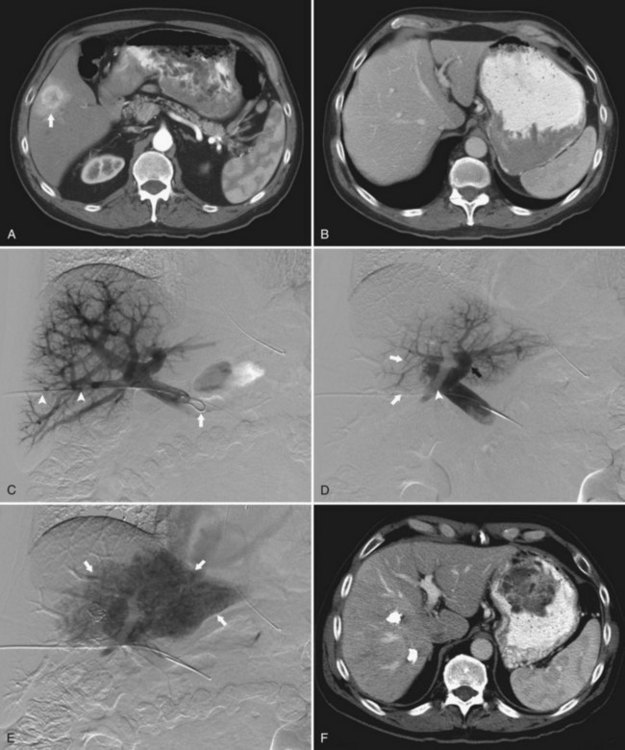
In the early 2000s, Madoff and coworkers (2003, 2005b) described a technique using angiographic catheters commercially available worldwide (Figs. 93B.2 and 93B.3). Under sonographic guidance, a 22-gauge Chiba needle (Neff Percutaneous Access Set; Cook Medical, Bloomington, IN) is used to puncture a distal branch of the right portal system. Subsequently, a 5- or 6-Fr vascular sheath is advanced over a guidewire into the right portal vein branch to aid with subsequent catheter exchanges. Flush portography is performed with a 5-Fr angiographic flush catheter placed within the main portal vein. Anteroposterior and craniocaudal projections are obtained as needed to delineate the portal anatomy.
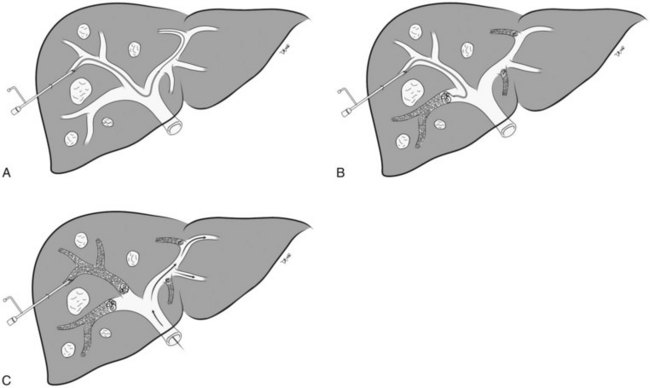
When embolization of the right portal vein is extended to segment IV (Fig. 93B.4), segment IV embolization should be performed first (Madoff et al, 2005b). This sequence is advocated because of the potential difficulty of exchanging catheters through a previously embolized right portal system and the possible dislodgement of embolic material from the right liver during the subsequent treatment of segment IV, which is usually embolized with a 3-Fr microcatheter placed coaxially through a selective 5-Fr angiographic catheter.
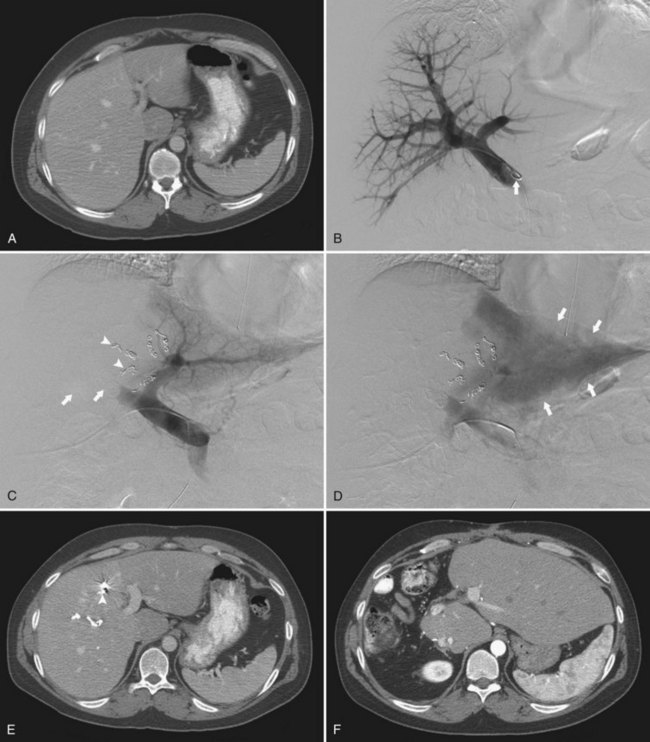
Early on, polyvinyl alcohol (PVA) particles (Contour SE Microspheres; Boston Scientific, Natick, MA) were the embolic agents of choice (Madoff et al, 2003). PVA was administered in a stepwise fashion: smaller particles (355 to 500 µm) were used first to occlude the distal branches, and larger particles (up to 1000 µm) were used subsequently to occlude branches more proximally. Larger particles were not used until the forward portal blood flow was considerably reduced. Additional embolization with the larger particles was then performed, until near complete stasis was achieved. Later, with the advent of spherical embolic agents, tris-acryl gelatin microspheres (EmboGold Microspheres; Biosphere Medical, Rockland, MA) became the embolic agent of choice (Madoff et al, 2005b). EmboGold microspheres ranging from 100 to 700 µm in diameter are administered in a stepwise fashion, similar to the method used for the PVA particles. After particulate embolization is complete, platinum microcoils (Boston Scientific) are placed within the proximal segment IV branches to further reduce portal blood inflow that could lead to recanalization.
Percutaneous Transhepatic Contralateral Approach
The percutaneous transhepatic contralateral approach was first described by Kinoshita and coworkers (1986) to slow the progression of tumor thrombus within the portal system. Modifications of this technique were later developed for the purpose of causing FLR hypertrophy (de Baere et al, 1993, 1996; Figs. 93B.5 and 93B.6
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


