and Andrea Bischoff1
(1)
Pediatric Surgery, Colorectal Center for Children Cincinnati Children’s Hospital, Cincinnati, OH, USA
Significant advances had been achieved in the field of prenatal diagnosis in general, as a consequence of amazing developments in the imaging technology. The use of ultrasound to visualize the fetus in utero already meant a great step in the diagnosis of gross malformations in utero [1–8]. Subsequently, the MRI amplified the possibilities of making much more accurate diagnosis of multiple congenital defects [9–11].
At the present time, we cannot claim that we can make accurate prenatal diagnoses of anorectal malformations. More specifically, we cannot determine the precise type of defect that the fetus has. Yet, with the current technology, we can make gross diagnoses that allow us to make important decisions and formulate meaningful recommendations [12–19].
The benefits of the prenatal diagnosis in anorectal malformations, as well as in all defects, include the possibility of giving the parents a fairly accurate idea of the functional prognosis of the future baby, which will influence his/her quality of life. This, beyond ethical and moral issues, will help the parents to make important decisions related to the possibility of terminating the pregnancy. In addition, depending on the specific type of defect, as well as its complexity, we can advise the parents as to the best possible place where the baby should be delivered, in order to receive optimal, comprehensive, and high-quality care. In some of the most serious anorectal and urogenital malformations, the therapeutic decisions taken during the first few hours or days of life are crucial for the future of the baby. Some mistakes that occur in the early management of these babies may have important repercussions for the future quality of life of the baby. That is the reason why in cases of complex defects that affect the colorectal area as well as the urogenital tract, we must advise to deliver the baby in a specialized center, where a multidisciplinary team of experts, with the necessary experience in that field, takes care of him/her.
3.1 Male Fetuses
A frequent in utero finding in babies with anorectal malformations is the presence of a dilated bowel (Fig. 3.1). This is a nonspecific finding that can be present in other conditions such as Hirschsprung’s disease.

Fig. 3.1
In utero MRI showing a dilated bowel in a fetus with anorectal malformation. Arrow shows the dilated bowel
The presence of intraluminal calcifications makes the dilated bowel sign more significant, since we know that the mixing of urine with meconium frequently produces calcifications (Fig. 3.2). We must keep in mind that over 80 % of the patients with anorectal malformations have a rectal urinary fistula, and meconium may go into the urinary tract as well as urine into the rectum.

Fig. 3.2
Intraluminal calcifications. In utero image. This is a consequence of the mixing of urine with meconium. Arrow shows calcifications
There are several signs that can be clearly seen by ultrasound and particularly with an MRI study that will make the diagnosis of anorectal malformation more likely. These signs include:
3.1.1 Abnormal Sacrum (Fig. 3.3)
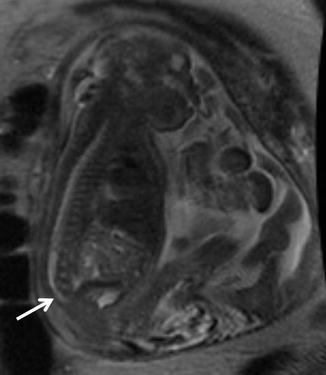
Fig. 3.3
In utero image of an abnormal sacrum. Arrow shows a very short sacrum
Thirty percent of the patients with anorectal malformations have an abnormal sacrum (see images in Chap. 6). These abnormalities may include a simply short sacrum, absent vertebra, as well as hemivertebra. Some patients may have a hemisacrum which is associated with a presacral mass.
3.1.2 Tethered Cord
This spinal cord defect is present in about 25 % of patients with anorectal malformations (see Chap. 23). A prenatal diagnosis is feasible as demonstrated in this figure (Fig. 3.4). This defect, as well as the abnormal sacrum, has a definite influence in the future prognosis for the urinary function and bowel function.
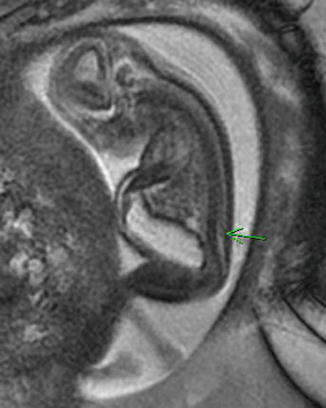
Fig. 3.4
Tethered cord diagnosed in utero. Arrow shows the low lying location of the conus
3.1.3 Absent Kidney (Fig. 3.5)

Fig. 3.5
Absent kidney in a fetus with anorectal malformation
It is the most common urologic malformation associated with anorectal defects (see Chap. 23). It is more commonly present in serious anorectal defects. The prenatal diagnosis is very reliable.
3.1.4 Vertebral Anomalies
A significant number of patients with anorectal malformations have an abnormal vertebra, mainly hemivertebra. This defect can be diagnosed in utero.
3.1.5 Hydronephrosis (Fig. 3.6)
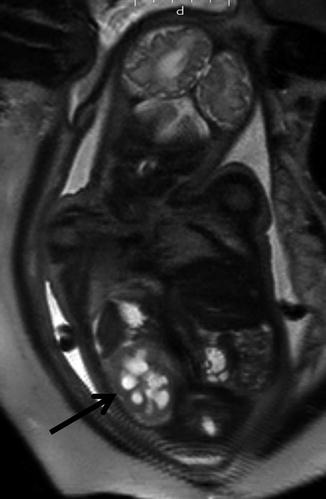
Fig. 3.6
Fetal hydronephrosis. Arrow shows the hydronephrosis
This is the second most common anatomic abnormality of the urinary tract seen in patients with anorectal malformations (see Chap. 23). Bilateral hydronephrosis denotes that both kidneys had been suffering in utero; therefore, we can anticipate a significant degree of kidney damage. This is extremely important because the patients will require special care to protect those kidneys already significantly affected.
3.2 Female Fetuses
3.2.1 Dilated Bowel and Intraluminal Calcifications
The presence of a dilated bowel is also seen in female patients. Intraluminal calcifications, on the other hand, are seen less often, since the majority of female cases do not have a communication between the rectum and urinary tract.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


