Figure 2.1
Renal CT-angiography showing the commonest finding of bilateral single renal artery
The primary role of the CT-angiography is to depict the vasculature of the kidneys since renal vascular anatomical variants are common [1]. The presence of 2–3 renal arteries does not preclude kidney donation but constitute an additional stress to both the kidney harvesting and the transplantation techniques (Fig. 2.2a, b). For the interest of this subject, we have chosen such a case in our description of the left nephrectomy. Many techniques have been described to avoid the need for a time consuming and stressful double arterial anastomosis in the recipient, including a Y-technique and a double gun-barrel fashion, however their description is beyond the scope of this book. On the other hand, it is generally accepted that the presence of more than three renal arteries is a contraindication for donor nephrectomy, and every effort should be made to find a “better” donor if the contralateral kidney does not offer a feasible vascular anatomy. CT-angiography allows one to exclude vascular abnormalities which constitute a contraindication to the living donor nephrectomy: renal artery stenosis and aneurysm, and fibromuscular dysplasia. The venous anatomy is equally important to be known and CT-angiography may reveal unusual presentation such as a retroaortic or a circumaortic left renal vein, both of which being manageable without much difficulty once anticipated. Axial CT-angiograms analysis allows also one to define the reno-azygo-lumbar venous arch and to be more cautious during dissection of the left renal vein inferior and posterior aspects.
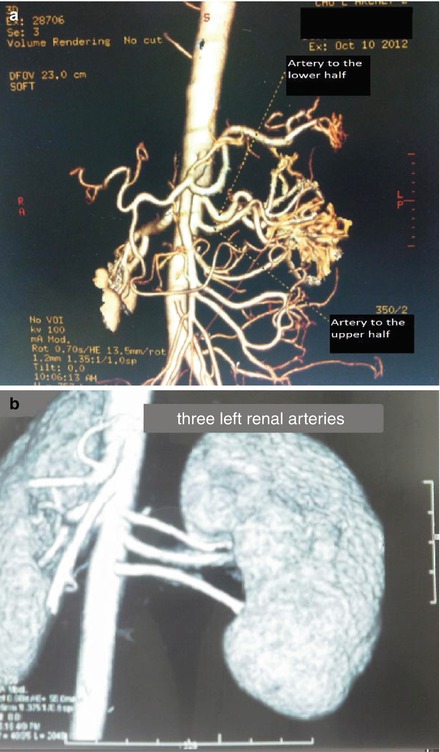
Figure 2.2
(a) CT-Angiography scan of the donor kidneys showing two arteries on the left side. Note the crossing-over resulting in the cranial artery supplying the lower half of the kidney and the caudal artery supplying the upper half. (b) Bilateral multiple renal arteries
Other benefits of the CT-angiography include visualizing the anatomy of the collecting systems and ureters, and detecting renal parenchymal abnormalities such as atrophy, cysts, scars, and tumors. It may also reveal renal stones, and extrarenal pathology, e.g. adrenal or gastro-intestinal tumors, inflammatory bowel disease, etc [2]. The tomodensitometry scan provides also an accurate evaluation of the kidneys volume which may show discrepancy with the values obtained from isotope renograms. Being projectional, the latter studies may indeed underestimate the function of a malrotated kidney, especially the right one.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


