Chapter 38 Postcholecystectomy problems
Overview
Cholecystectomy for gallbladder diseases has become the most common abdominal operation in Westernized countries. Since it was first performed in 1987, laparoscopic cholecystectomy (LC) has surpassed the open approach as the gold standard operation, largely because of significant decreases in operative time, patient pain, hospital stay, and costs (Begos & Modlin, 1994; see Chapter 34). At present, approximately 750,000 LCs are performed annually in the United States, accounting for roughly 90% of all cholecystectomies (Khan et al, 2007). This minimally invasive approach has revolutionized the treatment of patients with gallbladder disease and improved outcome, and it has permitted a liberalization of indications. Patients who would have otherwise been turned away from open cholecystectomy (OC) are now undergoing LC, and the open operation is now reserved for the most complicated scenarios (Khan et al, 2007).
Although LC has some advantages for both patients and surgeons, a new set of complications has arisen. The popularity of LC, combined with its innovative technology and the decreased threshold to whom it is offered, has resulted in novel postoperative problems, such as dropped stones, port-site hernias, and unique forms of common bile duct (CBD) injuries (see Chapter 42A, Chapter 42B ). More disturbing is that despite the widespread acceptance of LC and increasing experience with the procedure, it has a higher serious complication rate than that of the open approach. Furthermore, just as with open cholecystectomy, patients with abdominal pain that masquerades as gallbladder disease may undergo LC yet continue to be persistently symptomatic after the operation. This chapter addresses the causes of postcholecystectomy problems, both biliary and nonbiliary, along with optimal diagnostic and treatment strategies. Henceforth, we will refer to postcholecystectomy problems (PCPs) as persistent symptoms after surgical removal of the gallbladder regardless of etiology.
Indications for Cholecystectomy (See Chapters 30 and 31)
Gallstones that cause symptoms of epigastric and/or right upper quadrant (RUQ) pain, usually occurring after fatty meals and associated with dyspepsia and sometimes excessive flatulence, are most commonly treated with cholecystectomy. LC is successful in eliminating pain in 85% of patients with this constellation of presurgical symptoms (Tantia et al, 2008). Furthermore, patients with acute cholecystitis manifested by fevers, RUQ pain, elevated white blood count (WBC), and nausea and vomiting are also treated with LC.
A more contentious indication for cholecystectomy falls into the category of functional biliary disorders. Patients with persistent episodes of prolonged RUQ pain who lack a defined organic etiology should be evaluated for a functional biliary disorder. This condition, commonly referred to as biliary dyskinesia, affects approximately 2.4% of patients with biliary pain in the absence of cholelithiasis and results from the impaired physiologic contraction of the gallbladder, leading to insufficient emptying and pain (Barbara et al, 1987). Various studies suggest that patients with motility disorders of the gallbladder may benefit from LC (Westlake et al, 1990; Chen et al, 2001). However, if the physiologic derangement is downstream of the cystic duct, pain may persist even after removal of the gallbladder. This nebulous condition is termed sphincter of Oddi dysfunction, and it will be discussed in more detail later in this chapter. Finally, carcinoma of the gallbladder is an uncommon problem—only 9250 new cases of gallbladder cancer occurred in the United States in 2008—that is optimally treated with cholecystectomy and en bloc partial hepatectomy; but it is associated with a poor prognosis, with 5-year survival rates between 5% and 10% and an overall median survival of 3 to 6 months from diagnosis (Hueman et al, 2009). An in-depth discussion of these indications for cholecystectomy is found in Chapters 30, 31, and 49.
Complications of Cholecystectomy
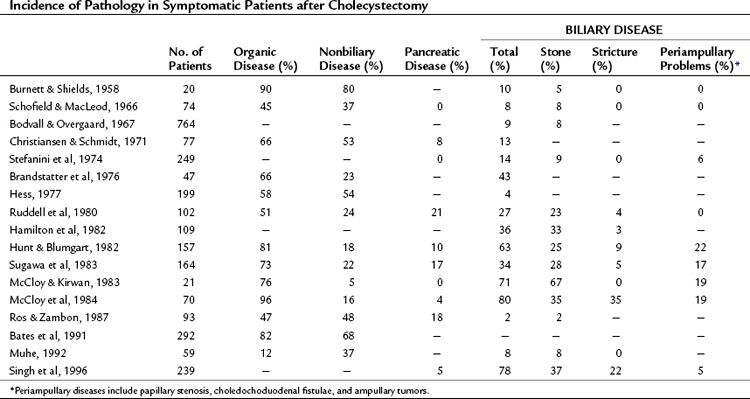
Postsurgical complications may be classified by biliary and nonbiliary causes. Furthermore, biliary complications may be subdivided into early, late, and mechanical (Table 38.1). Despite the advantages in care offered by the laparoscopic approach, cholecystectomy should still be recognized and referred to as a major operation. This is emphasized by the fact that mortality rates after cholecystectomy exceed many elective operations felt to be far more significant in scope, such as cardiac bypass, colonic resection, and even pancreatectomy. In a multivariate comparison of postcholecystectomy complications studied by Jatzko and colleagues (1995), open cholecystectomy was associated with higher morbidity (7.7% vs. 1.9%) and mortality rates (5% vs. 1%) than those of LC. The incidence of pathology seen in patients who are symptomatic after having a cholecystectomy is summarized in Table 38.2.
Table 38.1 Classification of Causes of Postcholecystectomy Symptoms
| Biliary |
| Early |
| Late |
| Mechanical |
| Nonbiliary |
Early Complications
Biliary Injury
Despite the advantages of LC over OC, common bile duct injuries are seen more frequently in the laparoscopic approach (0.2% to 0.7%) than in OC (0.1% to 0.04%) (Konsten et al, 1993; Nuzzo et al, 2005; Soderlund et al, 2005; Ali et al, 2007; Karvonen et al, 2007). Retrospective analyses of CBD injuries reveal that the two most common factors associated with injury are acute cholecystitis, wherein the normal gallbladder and biliary anatomy is obscured or distorted because of indurated and/or edematous tissues, and misperceptions or inexperience on the part of the surgeon. A learning curve is also implicated. In a series of 350 LCs reviewed by Huang and colleagues, CBD injuries occurred more often in the first 10 to 15 operations performed by a surgeon (Huang et al, 1993). In addition to the classic direct CBD injuries caused by misidentification of the cystic and common bile ducts, clipping of the “tented” CBD may occur in cases specific to LC when applying the first clip on the cystic duct by excessive traction of the CBD into the clip itself (Fig. 38.1). These injuries can lead to stricture and obstruction of the CBD and may be avoided by placing the first clip with visualized distance from the cysticocholedochal junction (Duca et al, 2003). In a retrospective review of 10,000 patients undergoing LC in a single center by four separate surgeons with no documented CBD injuries, it was found that surgical experience, preoperative imaging, precise operative procedures, and conversion from LC to OC when needed are necessary prophylactic measures to prevent CBD injuries (Ou et al, 2009). In addition, regular reliance on the “critical view” technique, along with abandonment of the infundibular dissection approach, can optimize a safer dissection (Strasberg et al, 2000; Strasberg, 2002).

Minor biliary leaks from the bed of the gallbladder, so-called Luschka leaks, may also be troublesome intraoperatively. Often, such leaks occur as a result of errant dissection into a deep plane of hepatic parenchyma. Accessory bile ducts found in the gallbladder bed may be controlled by ligation when transection and spillage is identified, but if these leaks are not identified in the operating room, postoperative bilomas and even bilious ascites may ensue. If the drainage of these “minor” leaks exceeds 500 mL over a 24-hour period, endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and transampullary stenting is useful in decompressing the biliary system and preventing reoperation (Pinkas & Brady, 2008; Pawa & Al-Kawas, 2009).
Hemorrhage
In a retrospective analysis of 9542 consecutive LCs by Duca and colleagues (2003), intraoperative hemorrhage occurred in 224 patients for an incidence of 2.3%. Bleeding was most commonly from the gallbladder bed and was treated with a fibrin-collagen patch. Conversion to an open procedure with suturing of the gallbladder peritoneum was required in five patients, however. It was noted that such hemorrhage from the gallbladder bed was encountered most commonly in patients with acute cholecystitis or cirrhosis. Tangential lesions of the cystic artery or, less commonly, total sectioning of the cystic artery occurred in 95 cases. In the majority of cases, the intraoperative bleeding was controlled laparoscopically with hemostatic clips, but conversion to an open procedure occurred in one patient. Damage to the hepatic artery occurred in one patient and required immediate open conversion. Finally, bleeding from the greater omentum was seen in 18 patients and was controlled laparoscopically in 16 patients.
Another source of massive intraoperative blood loss is from inadvertent incursion into a deep plane of hepatic parenchyma, where distal tributaries of the middle hepatic vein may be encountered. In fact, 10% of patients harbor large branches of the middle hepatic vein directly adjacent to the gallbladder fossa, which may lead to significant hemorrhage in instances of even minimal parenchymal dissection (Ball et al, 2006). Furthermore, postoperative hemorrhage may occur from trocar placement, or the bleeding may be from the cystic artery itself, albeit less than 1% of the time (Marakis et al, 2007). Finally, it should be recognized that management of profuse bleeding during LC, particularly when unexpected, can be fraught with significant ramifications that include major vascular ligation (hepatic artery, portal vein) and/or bile duct injury. This occurs from haphazard clip application or aggressive use of cautery in a poorly visualized field, thus conversion to open laparotomy is often the more prudent approach.
Dropped Stones
In 6% to 40% of LC procedures perforation of the gallbladder with subsequent spillage of gallstones occurs (Helme et al, 2009). These stones are usually retrieved under direct visualization, and the Morison pouch can be copiously irrigated; however, in 13% to 32% of patients these stones may be “lost” (Helme et al, 2009). This scenario contributes to postoperative morbidity 0.1% to 6% of the time, and the effects may vary in presentation and timing (Hand et al, 2006). Although such complications are infrequent, the patient may have symptoms such as fever, chronic abdominal pain, and/or intestinal obstruction. Furthermore, a meta-analysis by Zehetner and colleagues (2007) revealed that complications from “dropped stones” may present months to years after LC, most commonly as subcutaneous or intraabdominal abscesses or fistulas to less frequent manifestations such as liver abscesses or bacteremia. Additionally, stones have also been reported to erode into the chest cavity, causing empyema and broncholithiasis with expectoration (Zehetner et al, 2007). Perforation of the gallbladder during LC often occurs as the organ is dissected off of the liver by excessive retraction, direct puncture, or during omental adhesiolysis, but it may also occur as the gallbladder is being removed through trocar sites. Regular use of a retrieval bag may decrease complications from removal through trocar sites. Iatrogenic perforation of the gallbladder occurs more frequently in LC compared with OC; furthermore, spilled stones are arguably better visualized and more readily retrieved during open operations.
In a large retrospective review of more than 10,000 LCs, Schafer and colleagues reported a 6% incidence of gallbladder perforation with complications from dropped stones in 0.08% (Schafer et al, 1998). Furthermore, a 3-year prospective study by Rice and colleagues (1997) of 1059 patients who underwent LC at the Mayo Clinic revealed a perforation rate of 29% with an 11% dropped-stone rate. In this study, 2% of patients with perforated gallbladders developed subhepatic abscesses, and patients with intact gallbladders extracted had abscesses (Rice et al, 1997). In experimental studies using rabbit, rat, and dog models, the intraperitoneal introduction of gallstones resulted in a predominantly benign course without long-term complications (Welch et al, 1991; Sax & Adams, 1993; Cline et al, 1994; Cohen et al, 1994; Johnston et al, 1994; Zisman et al, 1995; Tzardis et al, 1996). Therefore, when gallbladder perforation and dropped stones are encountered, efforts should be made to retrieve stones with suctioning or forceps, and the subhepatic fossa should be copiously irrigated. Conversion to an open procedure is not necessary owing to a low rate of complications; however, it is a good policy to document the event and to inform the patient that stone spillage occurred.
Insufficient Cholecystectomy
In patients with severe acute inflamed cholecystitis, visualization of the cystic duct can be difficult, and historically this was treated with subtotal cholecystectomy. This approach has been proven to be effective and safe in open procedures. Recent reports suggest that when a critical view is impossible to obtain, laparoscopic subtotal cholecystectomy is also relatively safe (Hobbs et al, 2006; Ji et al, 2006; Sharp et al, 2009). When the triangle of Calot cannot be safely dissected, transection and oversewing of the gallbladder neck with resection of the anterior wall of the gallbladder, leaving a small strip of posterior gallbladder wall, can be an option.
Although this is a viable albeit rare approach, PCPs requiring an invasive reintervention still occur (Pernice & Andreoli, 2009). In a study from the United Kingdom of 26 cases of laparoscopic subtotal cholecystectomy over a 3-year period, five patients underwent postoperative ERCP for persistent biliary leak (n = 4) or retained common bile duct stones (n = 1). One patient developed a subphrenic abscess and underwent reoperative laparotomy, and another patient who was critically ill before surgery died postoperatively. A completion LC was required for one patient with a gallstone in a retained pouch, and two patients developed port-site hernias (Philips et al, 2008). In cases mandating laparoscopic subtotal cholecystectomy, the procedure must be performed by experienced surgeons, a drain should be left at the level of transection, and if a posterior wall is retained, it should be coagulated. A late manifestation of “partial” cholecystectomy is a remnant gallbladder pouch with potential for retained stones or cholecystitis.
Infections
Postoperative infection after cholecystectomy is a rare event. In a 7-year study conducted by the Centers for Disease Control and Prevention, out of 54,504 patients, the rate of surgical site infections (SSIs) was significantly lower in the laparoscopic approach when compared with open surgery (0.62% vs 1.82%, P = .001); however, the pathogens that caused SSIs were similar in both groups (Richards et al, 2003). The pathogens identified included Enterobacter species, Escherichia coli, and Staphylococcus aureus. The majority of infections in the open approach were seen in superficial spaces; in the laparoscopic approach, the majority of infections were intraabdominal. As expected, the SSI rates were higher in patients taken to the operating room emergently or with an ASA of 3 or higher (Richards et al, 2003). That said, prophylactic antibiotics given preoperatively to any low-risk patient undergoing elective LC are not indicated as evidenced by several reported studies (Chang et al, 2006; Tocchi et al, 2000; Uludag et al, 2009).
Late Postoperative Complications
Months to years after undergoing a cholecystectomy, patients may be seen with abdominal pain that differs from the symptoms felt before surgery. The incidence of pain from abdominal incisions is higher in OC (9%) versus LC (5%) over a 6-month period as reported by Vander Velpen and colleagues (1993). Bile duct neuromas have also been reported as a cause of pain up to 45 years after cholecystectomy (Paquette et al, 2009). A randomized controlled study performed by Halm and colleagues with 1-year follow-up in the prelaparoscopic era demonstrated that incisional hernias complicated 2% (1 of 60) of patients undergoing OC with a transverse incision compared with 14% (9 of 63) with a midline incision (Halm et al, 2009). Muhe (1992) reported that 12% of patients developed incisional hernias or pain after OC compared with 2% after LC.
Strictures (See Chapter 42A, Chapter 42B )
Benign stenosis of the CBD is more common after LC, and 95% of the time, it is related to iatrogenic injury in the form of partial or total sectioning, clipping, or ligation (Kassab et al, 2006). The incidence of patients developing strictures after LC varies from 0% to 2.7% compared with 0.2% to 0.5% after OC (Deziel et al, 1993; Strasberg et al, 1996). Postsurgical benign strictures may also result from delayed thermal injury or intraoperative ischemic devascularization (Genest et al, 1986; Deziel et al, 1993). Additionally, choledochoduodenal fistula formation tends to manifest more commonly after such stricture formation. In the postoperative period, the problems caused by strictures may result in abdominal pain, fever, and jaundice. Cholestasis may lead to choledocholithiasis and recurrent cholangitis (Kassab et al, 2006). Malignant strictures after cholecystectomy should also be considered, as rare cases have been reported (Sharma et al, 2008). This indicates a misdiagnosis prior to the cholecystectomy.
Biliary strictures have historically been treated by surgical reconstruction via hepaticojejunostomy, although many studies have recently reported the safety and efficacy of endoscopic balloon dilation and/or stenting as a noninvasive method to treat such problems (Kassab et al, 2006; Gouma, 2007). Surgery is therefore reserved for major bile duct injuries or failure of endoscopic therapy. A more detailed discussion of both benign and malignant strictures can be found in Chapter 42A, Chapter 42B, Chapter 50A, Chapter 50B, Chapter 50C, Chapter 50D .
Retained Stones
The remnant of the cystic duct or gallbladder (in subtotal cholecystectomy) has historically been implicated as the source of pain, nausea, and vomiting in postcholecystectomy patients (Bodvall, 1973). Several theories as to the etiology of such symptoms, characterized as the cystic duct stump syndrome, have been hypothesized (Garlock & Hurwitt, 1951). An increase in choledochal pressure resulting in cystic stump distension, inflammation or stone obstruction within the remnant of the cystic duct or gallbladder, and an increase in the sphincter of Oddi pressure have all served as causes of postcholecystectomy problems (Bodvall, 1973). However, various studies have confirmed that symptomatic improvement only occurs when a stone is present in the CBD or cystic duct and is subsequently removed endoscopically or via operative reintervention (Hopkins et al, 1979; Mergener et al, 1999; Tantia et al, 2008). In general, persistent symptoms following a cholecystectomy in which no cholangiogram was performed warrants analysis of the liver function profile and/or noninvasive imaging with either ultrasound or MRCP to assess for retained stones. If CBD stones are present, therapeutic ERCP is suggested (Fig. 38.2). The comprehensive management of common bile duct stones is discussed in Chapters 35 through 37.

Papillary Disorders
The apparatus responsible for directing the flow of biliary and pancreatic secretions is the sphincter of Oddi, which consists of three segments of smooth muscle: 1) the CBD segment, which is about 10 mm in length; 2) the pancreatic segment, which is roughly 6 mm in length; and 3) the segment of the confluence of both the bile duct and pancreatic duct, which is intraduodenal and close to 6 mm in length (Bistritz & Bain, 2006). When constricted, this sphincter impairs forward flow of both bile and pancreatic juices.
Sphincter of Oddi dysfunction (SOD) continues to be a diagnostic dilemma, and its management is controversial. Many entities have been reported describing this phenomenon, including papillary stenosis, sclerosing papillitis, and biliary spasm. The pathogenesis of this disorder is incompletely understood but is thought to result from an increase in basal sphincter pressure resulting in an increase in CBD pressure and stasis from obstructed biliary and pancreatic flow (Funch-Jensen et al, 2006). Microlithiasis causing transient obstruction has also been implicated as a result of stasis in the CBD from sphincter dysfunction, but this has been shown in several studies to be of little consequence in postcholecystectomy pain (Quallich et al, 2002; Rashdan et al, 2003; Bistritz & Bain, 2006). Uncoordinated spasm of the sphincter of Oddi has also been shown to produce the classic symptoms of RUQ colic with elevated liver function tests (LFTs) and has been characterized as biliary dyskinesia (Chuttani & Carr-Locke, 1993), therefore SOD may be described as two separate mechanisms: stenosis and dyskinesia.
Sphincter of Oddi Stenosis
Sphincter of Oddi stenosis refers to a fixed constriction or narrowing of part or all of the anatomic structures of the sphincter of Oddi. The stenosis may result from the trauma of recurrent passing gallstones, repeated attacks of pancreatitis, the effects of iatrogenic instrumentation, or other nonspecific causes. These insults result in fibrotic changes that cause a noncompliant orifice and elevated resting pressures, correlating to symptoms that fall into the category of type I biliary SOD (Bistritz & Bain, 2006). Ampullary biopsies of 43% of patients with SOD show evidence of fibrosis and inflammation (Ponchon et al, 1995). In the postcholecystectomy patient, the resulting backpressure of “papillary stenosis” is compounded by the lack of a gallbladder, which could normally serve as a reservoir for increased pressure in the CBD (Bistritz & Bain, 2006).
Sphincter of Oddi Dyskinesia
Uncoordinated contraction and relaxation of the sphincter of Oddi results in transient obstruction of biliary and/or pancreatic secretions. This leads to an elevation of intraluminal pressure with a concurrent elevation of LFTs. An increase in frequency of phasic contractions and a paradoxical response to the administration of cholecystokinin (failure of relaxation) may also occur in patients with dyskinesia (Tanaka, 2002). Interestingly, there is a significant overlap in patients with biliary dyskinesia and other intestinal motility disorders such as irritable bowel syndrome or hypertensive lower esophageal sphincter disorder (Evans et al, 1995, 1997; Chan et al, 1997).
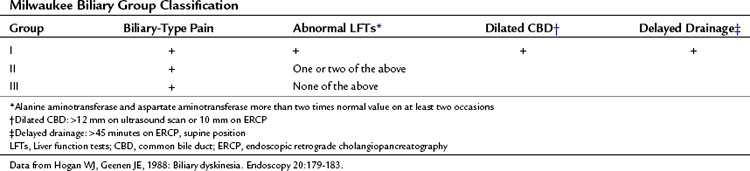
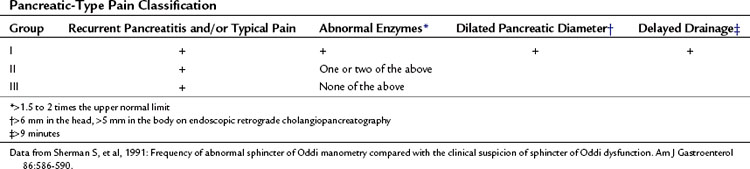
Clinically, SOD presents in 1% of patients after cholecystectomy and in 14% to 23% of patients presenting with the postcholecystectomy syndrome (Bar-Meir et al, 1984; Meshkinpour & Mollot, 1992; Drossman et al, 1993). SOD can also manifest as recurrent pancreatitis or with recurrent acalculous RUQ pain in patients with an intact gallbladder. Patients with SOD may be classified into three types based on presentation, laboratory results, and ERCP findings. Specifically, two classification systems, shown in Tables 38.3 and 38.4, stratify patients into three clinical groups for both biliary and pancreatic symptoms and predict the outcomes of endoscopic versus surgical treatment (Hogan & Geenen, 1988; Sherman et al, 1991). Patients with type I disease have biliary pain, elevated LFTs, an increase in the diameter of the CBD (>12 mm) with a delay in contrast drainage of more than 45 minutes. Patients with type II disease present with biliary pain and one or two of the remaining criteria delineated above. Patients with type III disease are seen initially with the sole criteria of biliary-type pain (Hogan & Geenen, 1988).
When patients present with the constellation of symptoms that fall under SOD, including pain that lasts at least 30 minutes, other organic causes of RUQ pain must be ruled out with laboratory tests that include complete blood counts and LFTs with amylase and lipase measurements. Transabdominal or endoscopic ultrasonography along with nuclear hepatobiliary scans and cholangiopancreatography may aid in narrowing the diagnostic differential. Often evidence of a dilated common bile duct is seen in the setting of type I SOD and is most amenable to treatment with sphincterotomy (Rolny et al, 1993; Sugawa et al, 2001
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


