Chapter 8 Pathology of Reproductive Endocrine Disorders
UTERUS
Endometrium
Endometrial Dating
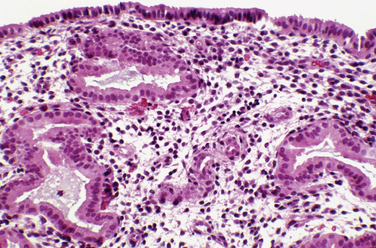
Most clinicians perform endometrial biopsy in the midluteal phase at about the time implantation is thought to occur. However, the original reports on secretory endometrial dating recommend a biopsy 3 days before the expected menses. Histologic criteria are then used to determine where the endometrial response would be in relation to ovulation (Table 8-1 and Figs. 8-1 and 8-2).
Table 8-1 Criteria for Histologic Dating
| Gland mitosis |
| Pseudostratification of nuclei |
| Subnuclear vacuoles |
| Edema |
| Stromal mitosis |
| Decidual reaction in stroma |
| Leukocyte infiltration |
| Secretion |
Several assumptions in the original concept of dating the endometrium besides the assumption of ovulation on day 14 increased the variation found with this method. For example, another assumption was that the length of the luteal phase is 14 days.1 In reality, there is a normal variation in luteal phase length of several days. In addition, the original description fixed the time of ovulation with the onset of the period after the biopsy. The onset of ovulation can be more accurately determined using current modalities, such as determination of the midcycle urinary luteinizing hormone surge or ultrasonic identification of the collapse of a follicle. The accuracy of the former is approximately 85%; of the latter, 95%. Additional intrinsic inaccuracies of dating resulted from intraobserver and interobserver variation. This variation is typically about 2 days. For these reasons, a 2-day difference between the histologic estimation and the actual interval since ovulation is considered within normal limits.
Recently a detailed analysis on endometrial dating demonstrated that the histologic criteria used are not as temporally distinct as originally thought, and thus do not provide an accurate method to detect a luteal phase defect. In one study, approximately 20% of fertile couples had a delay of more than 2 days.2 A between-cycle variation of more than 2 days was found in 30% to 60% of patients if the biopsy was performed between day 6 and day 13 after ovulation.
Endometrial Response to Exogenous Hormones
The endometrium responds to exogenous hormones with specific morphologic changes. With oral contraceptives, the progestin effect dominates because progestins decrease estrogen receptors. As a result, endometrial glands atrophy over time. The appearance of the stroma depends on the dose of progestin. Typically, a weak pseudodecidual response will occur (Fig. 8-3).
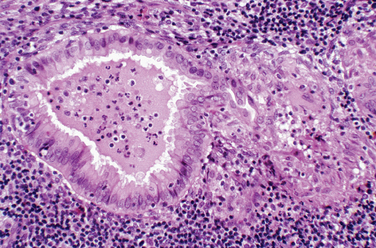
Endometritis
Chronic endometritis is sometimes demonstrated in endometrial biopsies for infertility or recurrent pregnancy loss. This is characterized by infiltration of plasma cells (Fig. 8-4). Chronic pelvic inflammatory disease, intrauterine devices, and postabortion complications are also associated with chronic endometritis. Although rare in the United States, endometrial tuberculosis may sometimes be found during a biopsy for infertility and is characterized by granulomas (Fig. 8-5).
Abnormal Uterine Bleeding
The biopsy of an endometrium for dysfunctional uterine bleeding in women may show a range of abnormalities of the endometrium (Fig. 8-6). In the reproductive age group organic lesions such as polyps and leiomyomas or a normal endometrium are often found. Pregnancy-related endometrial changes or premalignant or malignant changes may be found in this age group.
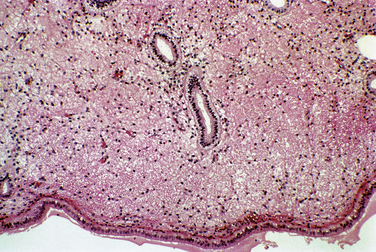
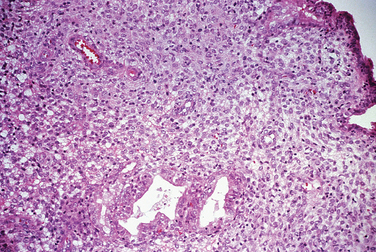
Pregnancy-related Endometrial Changes
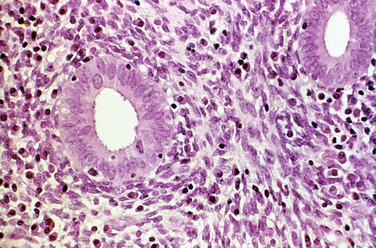
Early pregnancy, both intrauterine and ectopic, is characterized by hypersecretory endometrium (Fig. 8-7). However, hypersecretory endometrium is not specific for pregnancy, and similar changes can be seen with persistent corpus luteum cyst, double corpora lutea, or rarely as a drug effect. By the end of the first trimester, endometrial glands involute and the stroma shows a prominent decidual reaction (Fig. 8-8). Other histologic changes associated with gestation include the Arias-Stella reaction (Fig. 8-9) and optically clear nuclei (Fig. 8-10).
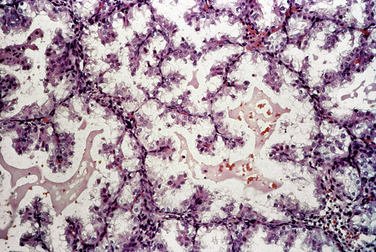
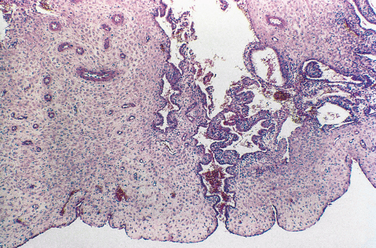
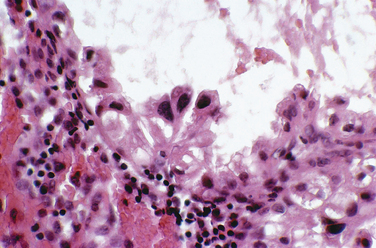
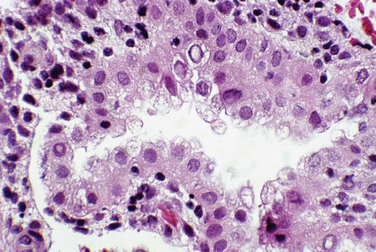
Figure 8-10 This endometrial gland has the optically clear nuclear appearance seen with pregnancy (center top).
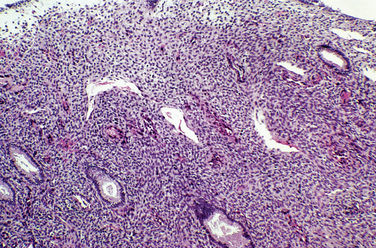
Endometriosis
Endometriosis is defined as the presence of endometrial glands and stroma at an extrauterine site. Although most commonly located in the pelvis, endometriosis can occur at a remarkable variety of extrapelvic sites (Table 8-2). Endometriotic lesions can invade neural tissue. The stromal component can undergo smooth muscle metaplasia. Hyperplasia of smooth muscle, especially the bowel, is characteristic.
Table 8-2 Reported Sites of Endometriosis Implants
| Lymph nodes |
Extrapelvic Locations
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|





