Chapter 27 Modern Concepts in Intrauterine Devices
INTRODUCTION
The intrauterine device (IUD) represents a unique approach to birth control and was the first woman-initiated contraceptive device to become widely available. From the beginning, it had the advantages of reversibility and relative effectiveness. In the past, these benefits were offset by the disadvantage of requiring placement by a healthcare provider, as well as by a spectrum of side effects and serious risks. Over the years, technological improvements have resulted in the evolution of the IUD into a highly efficacious and safe contraceptive method. Worldwide, it has become the most widely used form of reversible contraception. In Western Europe, 7% to 18% of women using contraception have an IUD.1 In the United States, less than 1% of women use an IUD for contraception, primarily because of reports of infectious complications resulting from IUDs no longer in use.2
HISTORY
It has long been alleged that the idea for a human IUD arose from Arab traders’ use of stones in the uterine cavities of camels to prevent unplanned pregnancies. Regretfully, this fascinating story appears to have no basis in fact.3 In actuality, the IUD appears to have evolved in the early 1800s from the stem pessary. This cup-shaped device had a stem that fit into the cervical canal and was designed to be placed in the vagina to support the uterus or rectum. It was soon found to have some contraceptive effectiveness, and in 1902 Hallwig designed a version with a stem that extended into the uterine cavity. This device, sold without prescription for self-insertion, was associated with a high infection rate and was not endorsed by the medical community.
In 1930 in Germany, Gräfenberg introduced a silver ring IUD without the tail common to earlier versions (Fig. 27-1). This contraceptive device had the drawback of a high expulsion rate. In 1934 in Japan, Ota modified this design slightly by adding a supportive structure to the ring. Both of these pioneers were ostracized by their respective medical communities. Regardless of their personal lack of success, their innovative work proved to be the first effective female-initiated contraceptive technique with a reasonably low risk of side effects and complications. Based on these attributes and a lack of equivalent alternative methods, IUD use gradually spread throughout the world.
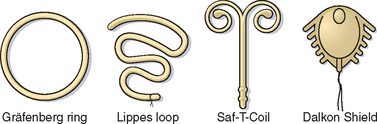
Intrauterine devices gained wide popularity in the 1960s and 1970s with the introduction of such models as the Margulies Spiral, the Lippes Loop, the Saf-T-Coil, the Birnberg bow, and the Dalkon Shield (see Fig. 27-1).4 In 1962, the Population Council convened the first International IUD Conference in New York City to analyze IUD data. In 1970, the Population Council published a report that concluded that IUDs were generally safe and an efficacious method of birth control.5 With this endorsement, IUD utilization increased rapidly. By early 1970, there were more than 70 IUDs on the market, which together made up 10% of the contraceptives used in the United States.
Inert IUDs
The IUDs approved by the Food and Drug Administration (FDA) in the 1960s and 1970s (e.g., Lippes Loop, Saf-T-Coil) were made of plastic (see Fig. 27-1). The pregnancy rates associated with the use of these IUDs were almost 20% per year. Another problem with this generation of IUD was that their relatively large size and shapes resulted in an unacceptable rate of increased menstrual bleeding and discomfort.
The Dalkon Shield
The Dalkon Shield was a uniquely designed IUD, whose associated complications resulted in the diminished popularity of IUDs in the United States that continues to this day. The Dalkon Shield, introduced by the A. H. Robbins Company in 1971, was a plastic ring to which had been added lateral spikes to decrease the expulsion rate, a central membrane, and a braided multifilament tailstring for removal (see Fig. 27-1). By 1974, more than 2.8 million women in the United States were using the Dalkon Shield. By coincidence, the early 1970s witnessed a period of increased sexual freedom referred to as the Sexual Revolution, which was associated with a corresponding increase in the prevalence of sexually transmitted diseases and pelvic inflammatory disease (PID).
The first indications of a problem were case reports of adverse IUD-related events, including PID, ectopic pregnancy, and septic abortions, some of which were fatal.6 Systematic investigations ultimately concluded that the Dalkon Shield, in particular, was associated with an increased risk of infectious complications. When tailstrings from different IUD models were cultured, the braided Dalkon Shield tailstrings were found to grow several types of bacteria, whereas monofilament tailstring from other IUDs had no positive cultures.7 This information supported the hypothesis that the increased risk of pelvic infection associated with the Dalkon Shield was the result of a wicking action of the braided tailstring that facilitated the ascent of bacteria into the upper genital tract. After only 3 years in production, the Dalkon Shield was taken off the U.S. market in 1974.
Copper-containing IUDs
Since the introduction of modern IUDs, research has focused on ways to increase their contraceptive efficacy, first by altering their configuration and then by including some pregnancy-preventing substance in their design. Studies in rabbits indicate that intrauterine placement of either copper or zinc could prevent implantation.8 Based on this information, copper-containing IUDs were developed for humans.
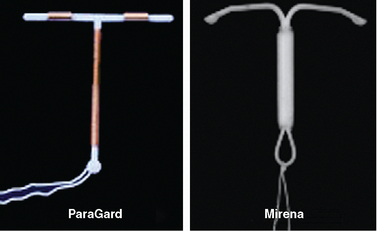
These first “medicated” IUDs had copper wire wrapped around the vertical stem of a T-shaped IUD. Earlier copper IUDs contained from 30 to 200 mm2 of copper.9 Animal studies indicated that adding higher amounts of copper dramatically enhanced contraceptive efficacy. The copper-containing ParaGard IUD, introduced in 1988, contains 300 mm2 of copper on the vertical arm and 40 mm2 on each of the horizontal arms, for a total of 380 mm2 (Fig. 27-2). This amount of copper decreased the pregnancy rate to less than 1% with copper. For the first time, the failure rate of an IUD was comparable to oral and injectable contraceptive methods and rivaled that of surgical sterilization. The ParaGard IUD is one of two IUDs currently available in the United States today.
The First Progestin-impregnated IUD
Hormone-impregnated IUDs were also evaluated to determine if they increase contraceptive efficacy. In 1976, the first progestin-releasing IUD was introduced to the market as the Progestasert. This T-shaped IUD had a vertical stem containing 38 mg of progesterone, which was released at a rate of 65 μg/day. In addition to contraception, it offered the additional benefit of diminished menstrual bleeding and discomfort. However, due to a failure rate of 2.9% and need for annual replacement, it was never widely utilized and its production was discontinued in 2001. The efficacy of this approach was greatly improved by the use of the more potent progestin levonorgestrel. The levonorgestrel-containing Mirena IUD is the second of two IUDs available in the United States today (see Fig. 27-2).
MODERN INTRAUTERINE DEVICES
Two IUDs are currently available in the United States; the copper T 380A (ParaGard, Ortho Pharmaceutical Corp., Raritan, N.J.) and the levonorgestrel intrauterine system (Mirena, Berlex Pharmaceuticals, Montville, N.J.) (see Fig. 27-2). Both are highly effective for preventing pregnancy with acceptable side effect profiles. The Mirena has the added benefit of decreasing both menstrual flow and discomfort in many patients.
The Copper-containing ParaGard IUD
The ParaGard IUD, introduced in 1988, has a flexible plastic T frame (see Fig. 27-2). A copper wire is wound around the stem, and copper sleeves are attached to the horizontal bars for a total copper surface area of 380 mm2. A monofilament tail-string is attached to the end of the vertical stem. The pregnancy failure rate for the ParaGard IUD is less than 1%, and it was originally approved by the FDA for 4 years of use before removal and replacement. However, subsequent studies showed that the ParaGard IUD could be used much longer without a decline in efficacy, and it is currently approved for 10 years of use. It has withstood the test of time with proven safety and patient tolerance.
The Levonorgestrel-containing Mirena IUD
The Mirena IUD was introduced in the United States in 2001. Also referred to as the levonorgestrel intrauterine system, the Mirena has a reservoir that contains 52 mg of levonorgestrel in the polyethylene T-shaped frame measuring 32 mm × 32 mm and has a monofilament string attached to the end of its vertical stem (see Fig. 27-2). The failure rate of this product is less than 0.1% per year. It has the added benefit of decreasing both menstrual bleeding and dysmenorrhea in most women.
Mechanisms of Action
The two IUDs currently available in the United States, the copper-containing ParaGard and the levonorgestrel-containing Mirena, both work primarily by inhibiting fertilization and secondarily by inhibiting implantation.10,11 Because they work before implantation, IUDs are not considered to be abortifacients. Both IUDs share a foreign body mechanism of action, but each has a second mechanism of action related to the substance they release locally.
Foreign Body Effect
Like earlier inert IUDs, both the ParaGard and Mirena IUDs produce a strong foreign body inflammatory reaction in the endometrium. The presence of the plastic T-shaped IUD causes the endometrial lining to release white blood cells, prostaglandins, and enzymes.12 In addition to making the endometrium unfavorable for implantation, this inflammatory reaction is toxic for sperm. As a result, IUD users have fewer sperm reaching the site of fertilization in the ampullary region of the fallopian tube.13 Based on studies of the earlier inert IUDs, it can be extrapolated that this foreign body reaction prevents pregnancy with a failure rate of approximately 20% per year. The addition of copper and progestin is responsible for further reducing the failure rate with modern IUDs to less than 1% per year.
Copper Effects
The primary contraceptive effect of the copper released from the ParaGard IUD appears to be toxicity to sperm and oocytes before fertilization in various locations in the uterus and tubes. In the cervix, a high copper concentration in the mucus decreases both sperm motility and the ability of sperm to penetrate the mucus.14–16 Copper has the curious ability to cause the heads and tails of sperm to separate.17
In the uterine cavity, copper ions enhance the inflammatory intrauterine response in the endometrium, adding to the spermicidal effect.10 In the fallopian tubes, high copper concentrations interfere with transportation and function of both sperm and oocytes.18 When the uterine tubes of women with a copper IUD in place were flushed, only half as many oocytes were present compared to controls, and none of these oocytes showed normal development.19
Copper also appears to affect fertilization and implantation. Although copper IUDs do not prevent ovulation, oocyte fertilization is decreased by half and those embryos that do form rarely implant.12,13 Further evidence of the preimplantation nature of copper IUD effects is the finding that serum levels of β-human chorionic gonadotropin (hCG) are uniformly undetectable in these women.20 To date, there has been no evidence to indicate that copper IUDs act as abortificients after implantation.
Levonorgestrel Effects
The levonorgestrel in the Mirena IUD has some contraceptive effects that are similar to copper but other effects that are unique. In the cervix, levonorgestrel, like copper, decreases sperm motility and the ability of sperm to penetrate the mucus, apparently by increasing mucus viscosity.11 This appears to be both a direct effect of the progestin on cervical mucus production as well as an indirect effect through alterations in ovarian function.
Levonorgestrel affects ovarian function.21 Part of the effect on cervical mucus appears to be secondary to the ability of levonorgestrel to suppress ovarian estrogen production. In some women, follicular development and ovulation is diminished, although most women remain ovulatory after the first year of use.22 Like copper, levonorgestrel also prevents fertilization by inhibiting transport of the sperm through the fallopian tube.
In contrast to copper, levonorgestrel prevents implantation by directly suppressing the endometrial lining. In addition to foreign body reaction, endometrial biopsies from levonorgestrel IUD users reveal atrophic endometrial glands and decidualized stroma consistent with a progestin effect.23 As with copper IUDs, evidence of the ability of levonorgestrel IUDs to prevent implantation is the finding that serum levels of β-hCG is uniformly undetectable in these women.24 Once again, there has been no evidence to indicate that levonorgestrel IUDs act as abortificients after implantation.24
Contraceptive Efficacy of Modern IUDs
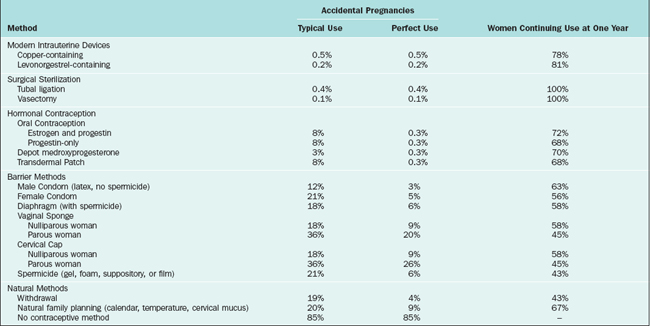
The annual and long-term pregnancy rates of the copper and levonorgestrel IUDs are among the lowest for available reversible contraceptive measures (Table 27-1). The 1-year pregnancy rate for the copper-containing ParaGard IUD is approximately 0.5 per 100 women.12 The 1-year pregnancy rate for the levonorgestrel-containing Mirena IUD is 0.2 per 100 women, but the overall 5-year pregnancy rate averages 0.7 per 100 women.25 These pregnancy rates do not appear to be affected by parity.
Table 27-1 Contraceptive Failure Rate for Various Methods During the First Year of Typical and Perfect Use, and the Percentage Continuing Use at the End of the First Year72,73
In practice, the cumulative pregnancy rates for both IUDs are impressively low. In a clinical study of use of these IUDs by 4000 women, the World Health Organization (WHO) reported the cumulative pregnancy rate for the Mirena IUD after 6 years to be only 0.6%, which was significantly lower than the rate for the ParaGard IUD, 2.0% (Table 27-2).26
Table 27-2 The Cumulative Six-year Probability of a Woman Discontinuing the Copper-containing ParaGard IUD and Levonorgestrel-releasing Mirena IUD26
| Name | ParaGard (copper) | Mirena (levonorgestrel) |
|---|---|---|
| Cumulative Pregnancy Rate | 2.0% | 0.6% |
| Intrauterine pregnancy | 1.8% | 0.6% |
| Ectopic pregnancy | 0.1% | 0.0% |
| Expulsion | ||
| Complete expulsion | 1.7% | 3.0% |
| Partial expulsion | 6.6% | 4.9% |
| Pelvic Inflammatory Disease | 0.0% | 0.3% |
| Menstrual Reasons | 10.7% | 36.2% |
| Amenorrhea | 0.6% | 23.8% |
| Reduced bleeding | 3.0% | 11.2% |
| Increased bleeding | 7.0% | 5.6% |
| Pain | 5.9% | 5.2% |
Use of Copper-containing IUDs for Emergency Contraception
Placement of the copper-containing ParaGard IUD in women after unprotected sexual intercourse is relatively effective in preventing subsequent conception. When used in this way for emergency contraception, the ParaGard IUD is most effective when placed within 72 hours after intercourse, but is still effective when placed within 5 days. In a meta-analysis of 20 studies of emergency contraception, the ParaGard IUD, with a subsequent 0.1% pregnancy rate, was found to be more effective than the standard oral contraceptive regimen, which had a 1.5% pregnancy rate.27
Discontinuation Rates
Discontinuation rates are important, because women who discontinue their birth control method for side effects are at high risk for pregnancy. In the first year, more patients continue using IUDs than any other reversible contraceptive method. Although studies of modern IUDs have shown general patient satisfaction and safety, the reported discontinuation rate after 7 to 8 years of use varies from 28% to 73%, depending on the population28–31
For both types of modern IUDs, menstrual reasons are listed as the most common side effect resulting in IUD discontinuation (see Table 27-2).26 For the ParaGard IUD, this was most commonly increased bleeding, whereas for the Mirena IUD, this was most likely amenorrhea or decreased bleeding. Because of the high rate of amenorrhea for the Mirena compared to the ParaGard IUD (23.8 vs. 0.6%, respectively), the 6-year continuation rate was significantly lower for the Mirena (43.8%) compared to the ParaGard (66.6%).26
Pregnancies and pelvic inflammatory disease (PID) are very uncommon for both types of IUDs. Although the study described in Table 27-2 showed a higher cumulative pregnancy rate for ParaGard compared to Mirena (2.0% vs. 0.6%, respectively), a multicenter prospective 7-year randomized study of more than 7000 women reported equal pregnancy rates (0.2 per 100 women-years) and PID rates (0.6 to 0.7 per 100 women-years) for both types of IUDs.28 Rates for both of these complications were highest in the first year after insertion.
Relative Cost
Modern IUDs are among the most cost-effective contraceptive methods.32 When calculating the total cost of a method, an economic analysis must include the initial costs, including contraceptive medication or device plus the placement fee; costs of treating side effects (e.g., surgical complications, deep venous thrombosis, amenorrhea, or urinary tract infections); and the cost of unintended pregnancies.
According to one analysis, over a 5-year period the copper-containing ParaGard IUD was calculated to be the least expensive at only $540, whereas oral contraceptives cost approximately $1784 over this same time period.32 Although vasectomy and tubal ligation would certainly be less expensive over the entire reproductive life of a woman, surgical sterilization has the obvious disadvantage of limited reversibility. The extremely low initial costs of many nonmedical approaches are more than offset by the cost of unintended pregnancies.
Return to Fertility
After removal of an IUD for reasons other than PID, there is no measurable residual effect on fertility no matter how long the IUD was used.33 This is in contrast to depot medroxyprogesterone, where fertility is usually delayed a matter of months until the medication has been cleared from the woman’s system.34
NONCONTRACEPTIVE BENEFITS OF IUDS
Inert and Copper-containing IUDs
A reduced risk of endometrial cancer was an unexpected finding in women who used either inert or copper-containing IUDs.35 Multiple studies performed throughout the world suggest that the risk of endometrial cancer in IUD users is reduced by 30% to 50%. It has been proposed that IUDs exert their protective effect through local structural and biochemical changes in the endometrium that may decrease endometrial sensitivity to estrogen or increase sensitivity to progesterone. Some authors suggest that this association could be a reflection of selection bias, because inert and copper-containing IUDs are less likely to be used in women with menstrual abnormalities who may be at increased risk for endometrial cancer. However, the data appears convincing that the incidence of endometrial cancer is decreased in women who have used either an inert or copper-containing IUD.
Levonorgestrel-containing IUD
Physiology
Continuous levonorgestrel exposure significantly suppresses the endometrium. Light microscopy shows that the endometrium becomes thin because of glandular cell atrophy and stromal cell decidualization. In addition, there is visible reduction in the size and number of endometrial blood vessels. Electron microscopy reveals that levonorgestrel causes thickening of the basal lamina between the endometrial epithelial and persistence of the complex intercellular junctions between the epithelial cells, which normally loosen around the time of implantation.36
Abnormal Uterine Bleeding and Dysmenorrhea
Excessive or too frequent uterine bleeding impairs the quality of life for many otherwise healthy women. After infection and uterine malignancies are excluded, the most common medical treatment for excessive uterine bleeding is progestin administration. Unfortunately, progestins given systemically do not always resolve these problems because of inconsistent effects on the uterus or because patients do not tolerate them because of systemic side effects or the risk of complications (including increased breast cancer). As a result abnormal uterine bleeding or dysmenorrhea remain some of the most common indications for hysterectomy in the United States.37






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


