Chapter 85D Microwave ablation and emerging technologies for liver tumors
Overview
Hepatic malignancies are common, with more than 1 million diagnosed each year worldwide. Tumors can be primary, as with hepatocellular carcinoma (HCC) or intrahepatic cholangiocarcinoma (IHC), or they can be secondary, as with colorectal liver metastases (CLM), neuroendocrine malignancy, or metastases from other primary cancers, such as those of the breast or lung. Many patients come to medical attention with advanced disease that is not amenable to surgical therapy. Unresectable disease carries a poor prognosis, because systemic chemotherapeutic agents and radiation therapy have limited efficacy in treating many of these diseases. As a result of the limited treatment options in this particular patient population, liver-directed regional therapies have evolved that include selective internal radiation therapy (Cianni et al, 2009), transarterial chemoembolization (TACE) (Rathore et al, 2010), portal vein embolization (PVE) (Manizate et al, 2010), and ablative technologies.
Ablation is not a new concept; it has been used in medicine for more than 100 years, initially as a therapy designed for patients with unresectable lesions (Halsted, 1894); however, advancements in medicine have transformed ablation into an effective locoregional therapy with an improved perioperative profile for morbidity and mortality and options of performing the procedure using an open, laparoscopic, or percutaneous approach. It has evolved from injecting ethanol (Uflacker et al, 1986) to employing different energy sources, such as cryoablation (Iannitti et al, 1998), radiofrequency ablation (RFA) (Iannitti et al, 2002), and microwave ablation (MWA) (Simon et al, 2006) to achieve tumor destruction (see Chapters 85A through 85C). Current ablation therapies also provide the flexibility to perform procedures in an ambulatory setting to allow treatment of patients whose disease is not amenable to resection. The application of ablative technology does not necessarily preclude patients from future operations, nor does it compromise their chance for transplantation (Casaccia et al, 2009); however, complications resulting from ill-advised ablative procedures may complicate subsequent attempts at resection.
Thermoablation is an effective modality, because irreversible thermal destruction of tissue occurs when temperatures above 50° C are maintained for an interval of 4 to 6 minutes (Larson et al, 1996). Vaporization and carbonization occur when tissue temperature is raised rapidly to over 100° C. Effective ablation relies on an adequate margin around the lesion, ideally 1 cm, to ensure complete eradication of microscopic foci. Large ablation volume may require multiple applications of thermal energy.
Physics of Microwave Energy
MWA that achieves heat destruction of tissue involves both active and passive heating. The active heating process of microwave energy requires the presence of dielectric molecules, such as water, to function. MWA is an excellent option for thermal ablation of solid organs, such as the liver (Brace, 2009a, 2009b). Clinical microwave energy operates at a frequency of 900 MHz to 10 GHz (Fig. 85D.1), which is much higher than radiofrequency (460 to 480 kHz). As a dipole molecule, water is affected by the applied electromagnetic field broadcasted by the microwave antenna. This property is called dielectric permittivity (ε). Water molecules orient themselves to the rapidly changing polarity of the electromagnetic field, and vibratory energy generates heat production. This process is called dielectric hysteresis. Microwaves emit nonionizing radiation for heating, and this produces homogeneous heating within the field regardless of the tissue types; this distinguishes MWA from monopolar RFA in terms of mechanism of heating and makes it a clinically superior method for ablation. The passive phase of microwave heating is by conduction of heat beyond the active heating zone and is susceptible to local tissue factors, such as heat and current sinking, which will be discussed later in this chapter.
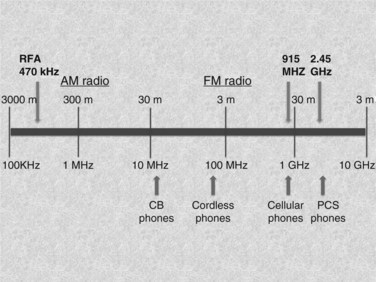
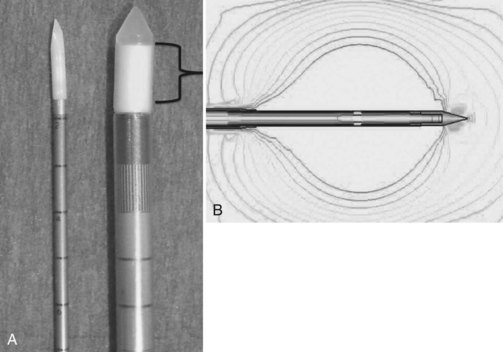
The MWA systems used in the United States today are 915 MHz, 2.45 GHz, and 9.2 GHz; however, only the 915-MHz and 2.45-GHz systems are commercially available for tumor ablation. The 915-MHz and 2.45-GHz systems are more effective for large tissue destruction than monopolar RFA, and the 915-GHz system is currently under investigation for ablating lesions in the breast. Microwave energy can be generated through a magnetron or solid-state amplifier (Brace, 2009a, 2009b), and the antenna broadcasts the electromagnetic energy to the target tissue. The coaxial cable consists of an inner and outer conductor, and dielectric material is placed between the two layers. At its tip, the outer conductor is stopped to expose the inner conductor for broadcasting the microwave energy (Fig. 85D.2). This inner conductor is covered in a ceramic pointed tip for insertion into the tissue, and microwave energy can pass freely through the ceramic. The power loss is influenced by power output, cable diameter, and antenna design. Given its broadcasting characteristic, the microwave system does not require a grounding pad.
Large ablative volume can be created by increasing the power and duration of the application. Several factors influence the final ablative size, including water content of the tissue, power output at the generator, power loss at the cable, antenna design, formation of clustered antennae, and the number of applications. Various tissue types exhibit different responses to microwave energy, and liver tissue usually exhibits a noticeable response to MWA (Hines-Peralta et al, 2006). Surgeons must understand the relationship between the different properties of tissue and the energy modality used to achieve successful ablation.
Local Tissue Factors That Affect Thermoablation
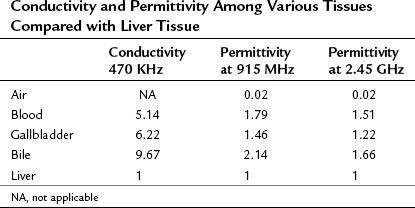
Coagulation necrosis of tissue is proportional to energy deposition minus heat loss (Goldberg et al, 2000). Hence, local tissue factors such as blood flow and tissue temperature affect energy deposition. Close proximity to blood vessels causes diversion of the current and decreases the amount of energy generated from the current; this is termed current sinking. The final ablative size is affected, because radiofrequency relies on heat transfer from the tip of the applicator, and the cooling from the vessel shunts the heat energy away; this phenomenon is termed heat sinking. Microwave technology also encounters such limitations but to a much lesser extent (Stauffer et al, 2003), because the propagation of microwave energy relies on the dielectric permittivity of the tissue, and it stays fairly constant along the broadcasted electromagnetic field (Table 85D.1). It can overcome the effect of current and heat sinking within its field and result in deeper heat penetration and more uniform ablative size. Outside the active heating zone, heat is propagated by conduction and is therefore susceptible to local factors such as heat sinking.
Another consideration is tissue desiccation and charring by the applicator during the heating process. Both conditions can significantly decrease the final ablative volume for RFA, because it requires a complete electric circuit to function. Acting as electric insulators, the resultant increase of impedance decreases the amount of current deposition and thereby decreases heat production. Moreover, if the target temperature is reached rapidly, above 100° C, the intracellular content vaporizes and carbonizes. The gas formation acts as an electric insulator that increases the impedance and hinders the heat diffusion (Dadd et al, 1996); both decrease the amount of current deposition and result in a less uniform ablative zone. Unlike radiofrequency, microwaves broadcast energy throughout the electromagnetic field and can achieve high power density uniformly, which results in deeper heat penetration and a more consistent ablative size.
915 MHz Versus 2.45 GHz
MWA, like RFA, can be carried out via three approaches: 1) open, 2) laparoscopic, and 3) percutaneous. The first clinical microwave system, Microtaze (Heiwa Electronics Industry, Tokyo), was developed in the 1990s. Clinical use was limited because of its 1.5-cm ablation zone (Saitsu et al, 1991, 1993), but 915-MHz and 2.45-GHz systems are currently available (Fig. 85D.3). Both systems were introduced to the United States market in 2008: the Viva Wave system (Valleylab, Boulder, CO) and the MTA microwave system (Microsulis Medical, Denmead, UK). Advancements in microwave technology and better antenna design have significantly improved ablative capabilities, and large-volume ablation can be reliably achieved.

The 2.45-GHz system is used more often in Europe and Asia, whereas the 915-mHz system is used in the United States; both are capable of producing an adequate ablation volume. The 2.45-GHz system uses a single antenna, and the 915-mHz employs a multiantenna array powered by separate generators. An advantage of using multiple antennae in different formations is to achieve various shapes and sizes of ablations (Simon et al, 2006). The microwave antenna is not composed of alloy but is coated with polytetrafluoroethylene (PTFE). It is not as rigid as the RFA metal applicator, and care should be taken during manipulation of the microwave antenna to prevent breakage at the tip of the antenna.
Technical Consideration for Performing Microwave Ablation
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


