Chapter 81B Metastatic malignant liver tumors
Neuroendocrine
Overview
The liver is second only to regional lymph nodes as the dominant site of metastases from all gastrointestinal (GI) tract malignancies. Because progression of hepatic metastases is the predominant cause of death in patients with GI cancers, hepatic metastases have been the focus of a multimodal treatment approach. Importantly, the accumulated experience documenting the survival potential of hepatic resection for selected patients with colorectal metastases (see Chapter 81A) has prompted evaluation of this approach for other malignancies metastatic to the liver. Whether similar approaches will prove effective for neuroendocrine metastases remains unclear.
Evidence supporting hepatic resection for metastatic GI neuroendocrine tumors (NETs) continues to emerge. Hepatic resection of metastatic NET to the liver is appealing because gastrointestinal NET has a similar route of metastatic dispersal through the portal venous system, as do colorectal cancers. Moreover, their natural history is typically prolonged compared with other GI tract cancers and, in fact, with other solid tumors. Initial experience with hepatic resection for metastatic NET (Foster & Berman, 1977) suggested that patients might benefit in terms of survival and symptom relief from clinical endocrinopathies when antihormonal and antineoplastic therapies were ineffective. Consequently, interest in hepatic resection for metastatic NET has grown. In addition to the prolonged natural history of NET and the clinically significant endocrinopathies, several other observations have supported further assessment of hepatic resection: 1) the prolonged presence of intrahepatic disease before evidence of extrahepatic progression, 2) the impression that the severity of clinical endocrinopathy correlates with the intrahepatic volume of metastatic disease, 3) the resectability of the primary and regional NET despite metastatic disease, and 4) the presence of normal, nonmetastatic liver. This chapter details the clinical data supporting hepatic resection for metastatic NET; presents the current outcomes for hepatic resection, hepatic transplantation, and ablative therapy for metastatic NET; and presents an algorithm for long-term management of patients with metastatic NET in the liver.
Classification of Gastroenteropancreatic Neuroendocrine Tumors
Most neuroendocrine metastases to the liver are of GI or pancreatic origin, so-called gastroenteropancreatic (GEP) tumors (Rindi et al, 1998). GEP neuroendocrine tumors have historically been divided into two broad types, carcinoid and noncarcinoid, either of which may or may not be associated with hormone production that causes a clinical endocrinopathy (functional or nonfunctional, respectively). Traditionally, GI carcinoids (GICs) have been classified by their site of origin—foregut (lung, thymus, stomach, duodenum, pancreas, bile duct, gallbladder, and liver), midgut (small intestine, appendix, and proximal colon), and hindgut (distal colon and rectum)—because biologic and biochemical features within these groups vary. In contrast, pancreatic neuroendocrine tumors have been classified simply by whether they are functional (see Chapter 61). Regardless of origin, neuroendocrine tumors are similar histopathologically. Many histologic and morphologic features are shared by both benign and malignant tumors. Importantly, only the confirmed presence of metastases confers an unequivocal diagnosis of malignancy.
Clinical behavior for NET has ranged from an indolent to an aggressive clinical course with rapid cancer progression and death. For GEP neuroendocrine tumors, two schemes have been employed (Capella et al, 1995; Solcia et al, 2000). Broadly these classifications stratify patients with malignant GEP into low-grade (well-differentiated) or high-grade (poorly differentiated) NET (World Health Organization [WHO] classification) and subtype each as either functioning or nonfunctioning. In general, only patients with liver metastases from well-differentiated (low-grade) but not poorly differentiated (high-grade) NET are approached surgically. The TNM (tumor-node-metastases) staging has also been proposed (Rindi et al, 2006, 2007) and correlated with survival (Fischer et al, 2008; Pape et al, 2008a, 2008b; Skov et al, 2008). Some classifications tend to limit patients based on the number and extent of hepatic metastases on the radiologic imaging: a single metastasis (type I), isolated metastatic bulk accompanied by smaller deposits (type II), and disseminated metastatic spread throughout the liver (type III). These three groups differed significantly in regard to tumor-related characteristics, but this classification correlated with therapeutic approach and long-term survival (Frilling et al, 2009). The recently published guidelines by the North American Neuroendocrine Tumors Society (NANETs) highlight the importance of a uniform approach to pathologic reporting. This is especially relevant regarding differentiation and grade of individual tumors, which have a major impact on prognostication and choice of therapy (Klimstra et al, 2010).
GIC cancers produce a variety of proteins and peptide hormones (Onaitis et al, 2000; Schnirer et al, 2003). Almost all NETs are positive for neuroendocrine markers chromogranin A and neuron-specific enolase, but serum levels have correlated poorly with prognosis (Tomassetti et al, 2001); however, they are useful for treatment follow-up (Jensen et al, 2007; Nikou et al, 2008). Pancreatic NETs produce a wide variety of one or more peptides: gastrin, insulin, glucagon, and vasoinhibitory peptide, among others (Gumbs et al, 2002; Mansour & Chen, 2004). Nonfunctional pancreatic NET implies either the production of an inactive peptide, subclinical hormone production, or no peptide production. Reviews for the specific endocrinopathies from pancreatic neuroendocrine tumors are cited for reference to recognize their implications in clinical management (Gumbs et al, 2002; Mansour & Chen, 2004).
Epidemiology
A brief overview of the most commonly encountered primary GEP NETs is presented because combined resection of the primary and regional extent of disease and hepatic metastases is frequently undertaken. GICs comprise nearly 75% of all carcinoids with the remainder primarily of bronchopulmonary origin. The distribution of GIC is composed of the small intestine (35%), rectum (23%), appendix (19%), colon (12%), stomach (6%), duodenum (4%), and hepatobiliary-pancreatic region (2%) (Modlin et al, 2003). The relative incidence of gastric and rectal carcinoids has increased over the last 3 decades but has decreased in the appendix. GICs are frequently associated with noncarcinoid tumors in the small intestine (29%), stomach (21%), and appendix (18%). Overall, localized disease characterizes the presentation of rectal (80%) and gastric (70%) carcinoids, and nonlocalized disease is represented in colonic (80%) and small intestinal (67%) carcinoids. Although GICs are often considered to behave benignly, 13% of patients have metastatic disease at presentation, and overall 5-year survival for GIC is only 67% (Kulke & Mayer, 1999).
Nonfunctional NETs of the pancreas have an equal sex distribution (Hochwald et al, 2001). NET of the pancreas occurs in 0.5 to 1 person per 100,000 population. Nonfunctional NET accounts for more than 50% of pancreatic NET in most series, and wide variations in incidence between types of NET are likely related to the definition of “nonfunctional.” Multicentricity is not infrequent (15%). The epidemiology of functional pancreatic neuroendocrine tumors varies widely, with or without the multiple endocrine neoplasia (MEN) 1 syndrome, and is beyond the scope of this chapter; however, references are provided.
Small Intestinal Carcinoids
Small intestinal carcinoids are the most common GIC (Kulke & Mayer, 1999; Modlin et al, 2003). Patients usually present with abdominal pain, diarrhea, GI obstruction, and bleeding. Small intestinal carcinoids account for 90% of patients with the carcinoid syndrome. Approximately 20% of patients with the syndrome will have clinically evident carcinoid heart disease, and an even larger proportion will have occult heart disease detectable by echocardiography (Bernheim et al, 2007). Small intestinal carcinoids are often associated with dense mesenteric fibrosis, intestinal obstruction, hemorrhage, and intestinal ischemia secondary to vessel compression by metastatic regional lymph nodes and local release of vasoactive hormones (mesenteric angiopathy) (Eckhauser et al, 1981). Nearly 20% to 30% of patients have multiple GI carcinoids, and more than a third of patients have concurrent noncarcinoid cancers. Besides regional lymph node metastases, these carcinoids frequently metastasize to the liver, peritoneum, retroperitoneal nodes, and ovaries.
Resection is the only potentially curative treatment for small intestinal carcinoids (Hellman et al, 2002a; Loftus & van Heerden, 1995; Soreide et al, 1992; Woodside et al, 2004). Because of the frequency of the associated syndrome, careful preoperative evaluation and preparation are necessary. When suspected clinically, baseline urinary 5-hydroxyindole acetic acid (5-HIAA) levels should be obtained. The extent and site of the primary small intestinal carcinoid can be defined by barium contrast GI series, enteric computed tomographic (CT) scan, enteric magnetic resonance imaging (MRI), or by small bowel enteroclysis. Further imaging of the abdomen and chest for metastatic disease is best defined by contrast-enhanced CT. Often CT will identify mesenteric adenopathy and stranding characteristic of regionally advanced small bowel carcinoids even without identification of the site of the primary carcinoid on small bowel contrast studies.
Assessment of the relationship of the regional lymphatic metastases to the vessels of the small bowel is important in planning resection of the primary and regional extent of disease (Mullen et al, 2005). Despite the typical desmoplastic reaction adjacent to the involved regional lymph nodes, resection is feasible, except with extensive invasion of the third portion of the duodenum and the uncinate process of the pancreas, circumferential arterial and venous encasement without patent proximal arterial collaterals, or distal mesenteric arteries not large enough for reconstruction (Ohrvall et al, 2000; Schindl et al, 2002).
Various imaging methods may be helpful. Although not anatomically useful in operative planning, somatostatin receptor scintigraphy and octreoscanning are useful is evaluating the overall disease extent and the site of the primary, when not recognized by other studies; these are also helpful in modifying treatment strategies (Slooter et al, 2001). The role of MRI is increasing, primarily in assessing the extent of hepatic metastases. MRI is particularly sensitive in detecting small metastases within the liver and often will detect disease not seen by other imaging techniques inclusive of CT; however, MRI has limited applicability for defining the site of the primary carcinoid.
The recognition of carcinoid heart disease demands a thorough cardiac evaluation (Fox & Khattar, 2004). The major implication of carcinoid heart disease is the presence of right heart failure and the consequently elevated systemic venous pressures that can cause a pulsatile liver (implying hepatic vein pressures >25 mm Hg), which precludes hepatic resection. The presence of clinical significant carcinoid heart disease dictates medical treatment, and occasionally even valve replacement, prior to resection of the primary small intestinal carcinoid and the hepatic metastases (Moller et al, 2005). Survival after surgical repair of carcinoid heart disease is improved compared with medical treatment, even without surgical treatment of hepatic metastases (Connolly et al, 1995). Some patients may be candidates for hepatic resection after repair of carcinoid heart disease, depending upon objective decreases in systemic venous hypertension and the degree of functional cardiac improvement (Connolly et al, 2002; McDonald et al, 1999). Conversely, hepatic resection has been shown to be associated with decreased cardiac progression of the carcinoid heart disease and improved prognosis (Bernheim et al, 2008).
Any patient with the carcinoid syndrome requires preoperative and intraoperative somatostatin analogue therapy to prevent a carcinoid crisis (Oberg et al, 2004), a clinical syndrome of life-threatening intraoperative hypotension or hypertension and severe flushing with or without concurrent bronchospasm or arrhythmias. To date, the frequency and factors predictive of this perianesthetic complication remain unknown. Prevention is essential, and appropriate treatment should be prescribed in all patients undergoing intervention for metastatic carcinoid tumors (Kinny et al, 2001). Short-acting analogues are preferred, even if the patient has received the long-acting analogue within 30 days. Management should consist of subcutaneous short-acting somatostatin analogue on call to operation and intravenous infusion of the analogue throughout the operation and in recovery. Additional intraoperative increases in infusion rates are appropriate for unexplained intraoperative hemodynamic instability.
Resection of small intestinal carcinoids should encompass the primary tumor, any multicentric tumors, and the regional lymph nodes. When intestinal ischemia is present, resection of the thickened, chronically ischemic bowel is indicated; resection of the regional lymph nodes is often possible by keeping the dissection immediately adjacent to the nodes and retracting the visceral vessels away from the involved nodes (Hellman et al, 2002a). Preservation of the blood supply to the GI tract is essential to prevent short-bowel syndrome. As mentioned previously, preoperative CT with intravenous contrast will define those patients with resectable nodal disease, which is very difficult to assess intraoperatively. Resection of hepatic metastases is generally indicated only if complete resection of the primary and regional disease is feasible. Resection of hepatic metastases should be performed concurrently, if all gross metastases can be excised. If nearly all of the hepatic disease can be resected (or ablated), cytoreductive resection should be considered, because both survival and symptom-free quality of life may be improved (Knox et al, 2004; Sarmiento et al, 2003; Chambers et al, 2008). Staged resections can be performed with similar expectations in outcomes. Overall 5-year survival for small intestinal carcinoid ranges from 50% to 67%.
Pancreatic Neuroendocrine Tumors (See Chapter 61)
An aggressive operative approach generally is warranted for NET of the pancreas (Fendrich et al, 2006; Hochwald et al, 2001; Matthews et al, 2002; Phan et al, 1998; Schurr et al, 2007; Solorzano et al, 2001). Resection remains the treatment of choice for patients with localized NET of the pancreas and for selected patients with hepatic metastases (Oberg & Jelic, 2008). Resection of the primary NET and the regional lymph nodes is generally possible despite their often large size. The extent and type of pancreatectomy is dictated by the site of the primary NET; pancreatoduodenectomy is used for NET of the head of the pancreas, and distal pancreatectomy/splenectomy is best for body or tail NET (see Chapter 62A, Chapter 62B ). In some cases, enucleation may be an alternative approach. For patients with locally invasive NET of adjacent structures or the GI tract, resection should be en bloc. Laparoscopic pancreatectomy is currently applicable for resection of most pancreatic NET (Fernandez-Cruz et al, 2002, 2008). Whether concurrent laparoscopic resection of the primary pancreatic NET and hepatic metastases is feasible has not been proven. Concurrent resection of primary pancreatic NET and hepatic metastases can be performed safely, although staged resections may be preferable, particularly in patients with involvement of the head of the pancreas (Sarmiento et al, 2002). Overall actuarial 5-year survival rates for NET of the pancreas range from 45% to 63% with a median survival of about 4 years.
Natural History
Regardless of whether NETs are classified as carcinoid or noncarcinoid, the natural history of patients with unresected or unresectable hepatic metastases has been similar. Overall, patients with unresected hepatic metastases from NETs have a 5-year survival of approximately 30% (Proye, 2001) and a median survival of 17 months (House et al, 2006).
Several factors affect the natural history of both carcinoid and noncarcinoid cancers (Durante et al, 2009). Clearly, liver metastases are the most significant factor adversely affecting outcome (Moertel, 1987; Pape et al, 2008a). With or without liver metastases from NET, 5-year survival is approximately 30% to 40% and 90% to 100%, respectively. Poorly differentiated NET and progressive neuroendocrine metastases in the liver (>25% volume increase on two CT scans within 3 months) further adversely affects survival among patients with hepatic metastasis (Madeira et al, 1998). Progression in size or number of hepatic neuroendocrine metastases can be expected in 90% after a median follow-up of 11.5 months (Skinazi et al, 1996). Carcinoid heart disease occurs only in the presence of metastatic carcinoid tumor to the liver independently and predicts poor survival. The survival of patients with clinically severe carcinoid heart disease is approximately 1.6 years; the survival rate is only 31% at 3 years, unless cardiac surgery is undertaken successfully (Connolly et al, 1995; Fox & Khattar, 2004). Patients with carcinoid heart disease should be considered for hepatic surgery, as stated before, because cardiac disease progression is reduced, and prognosis is improved (Bernheim et al, 2008).
Although uncontrolled functioning endocrinopathies from metastatic neuroendocrine tumors can be life threatening—for example, severe hypoglycemia from insulinoma and GI perforation from gastrinoma—the impact of such events on the natural history of these patients is unknown. Conversely, it is likely that clinical control of endocrinopathies can affect natural history of NET; however, specific studies to document clinical control of endocrinopathies by antihormonal therapy with objective tumor responses have not been well documented, except for gastrinoma before and after the use of H2 blockers or proton pump inhibitors (Norton et al, 2003a).
Similar to carcinoid tumors, the 5-year survival of patients with pancreatic NET ranges from 30% to 40% with a median survival of approximately 40 months (Chen et al, 1998; Thompson et al, 1985). Whether the presence or absence of clinical endocrinopathies affects the natural history of patients with metastatic pancreatic NET is unclear; however, the specific NET likely affects overall natural history. Up to 75% of patients who present with midgut or hindgut tumors are likely to have liver metastases, in particular the nonfunctioning group, and those with a pancreatic primary (likely to be high grade) have the highest rate of liver involvement (Steinmuller et al, 2008). In a series of 35 patients with hepatic metastases, 60% of which were from gastrinomas, the 5-year survival was approximately 70%. The prognosis also is affected by the extent of metastatic NET in the liver (Chamberlain et al, 2000; Phan et al, 1998); the 5-year survival was only 24% with more than 75% tumor replacement of the liver, whereas 5-year survival approached 80% for less than 50% tumor replacement.
Surgical and Ablative Treatment of Hepatic Neuroendocrine Metastases
Hepatic Resection for Neuroendocrine Metastases
The current mainstay of treatment for metastatic GI neuroendocrine tumors to the liver is resection (see Chapter 90E); however, no randomized controlled data support improved survival from hepatic resection of metastatic NET. Although hepatic resection of malignancy is employed most often with curative intent, the tumor biology of these typically indolent and slow-growing cancers renders them less responsive to more commonly employed palliative therapies, such as chemotherapy and radiation; thus, resection with palliative intent (cytoreduction) may afford patients a real and significant advantage in palliation and may prolong survival. Importantly, the focus on palliation and extension of life, rather than on complete remission, is conceptually a paradigm shift, because most hepatic resections are undertaken for cure in patients with metastatic solid cancers.
The treatment of hepatic metastases from NET is aimed at reduction of the mass of malignant tissue (cytoreduction) chiefly for two reasons: first and foremost, metastatic gastrointestinal NET is usually indolent and slow growing, with a well-differentiated histopathologic grade (WHO classification) (Solcia et al, 2000); thus chemotherapy and radiotherapy regimens targeted toward rapidly dividing cells are relatively ineffective; second, symptoms secondary to expression and secretion of biologically active peptides by these tumors is directly related to overall mass of tumor, although production of peptides may be heterogeneous among individual metastases. Similarly, pain and decreased performance status may negatively impact on quality of life for patients with nonfunctional NET metastatic to the liver. In patients who do respond to medical treatment, debulking surgery—cytoreduction of more than 90% of the liver tumors—is a valid and direct method of providing relief from symptoms. These reasons, coupled with improved safety for hepatic resection, have prompted some to advocate hepatic resection as a primary therapeutic option for patients with both functional and nonfunctional metastatic NET (Chambers et al, 2008). Based on these premises, hepatic cytoreduction, whether by hepatic resection or transplantation, should address clinical endocrinopathies and improve survival; as a corollary, the duration of response should be in proportion to the extent of the debulking or cytoreduction of the metastatic NET and the growth rate of the residual NET (House et al, 2006).
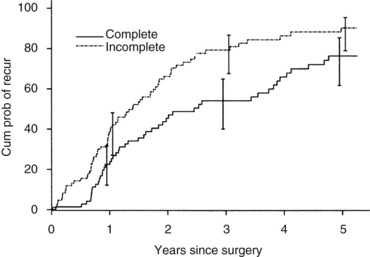
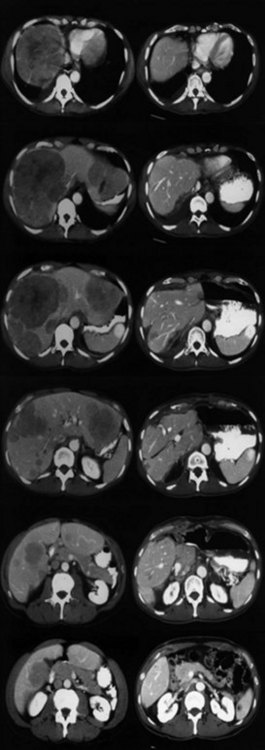
Currently, hepatic resection of metastatic NET is recommended if the primary tumor and regional disease are resectable or resected, and a minimum of 90% of the volume of hepatic metastases is resectable or ablatable (Steinmuller et al, 2008). Our initial results showed that debulking hepatic resection could be performed safely, and overall survival was about 75% at 4 years (Que et al, 1995). No significant difference in survival was found between patients undergoing complete (R0) or incomplete (R1 to R2) resections. Mean duration of symptom response was nearly 2 years. Subsequently, our findings in 170 patients undergoing hepatic resections showed that symptoms resolve in 98% of patients. Median time to symptom recurrence was 45 months, and 59% of patients experienced recurrent symptoms at 5 years. Overall survival was 61% and 35% at 5 and 10 years, respectively, and perioperative mortality rate was 1.2%. Recurrence, however, was 84% at 5 years and 94% at 10 years (Fig. 81B.1; Sarmiento et al, 2003). Examples of results obtained from cytoreductive hepatic resection for neuroendocrine tumors are shown in Figure 81B.2.
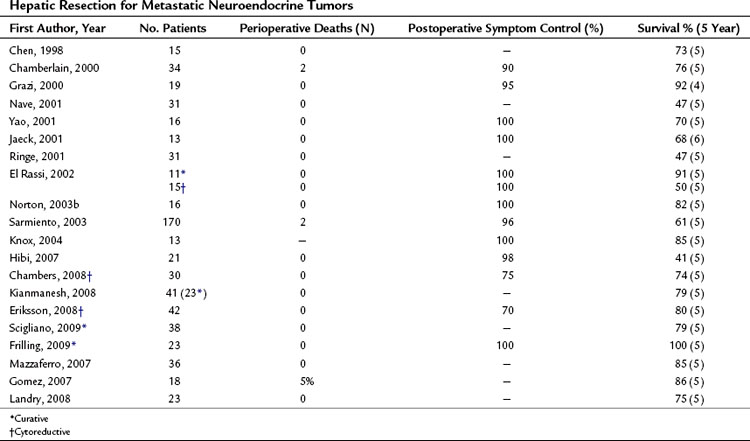
A review of the current literature on hepatic resection for metastatic NET is summarized in Table 81B.1. The cumulative findings from these reports support an aggressive operative approach for metastatic NET. Overall 5-year survival has ranged from 41% to 82% with a median 5-year survival of up to 100%. Only four perioperative deaths have been reported among the tabulated patients (n = 556). When addressed, resolution of endocrine symptoms exceeded 90% in most series, although duration of response was not routinely reported.
Although the majority of patients reported to date have had metastatic carcinoid cancer to the liver, survival has not differed appreciably among patients with carcinoid and noncarcinoid (primarily islet cell) cancers. Current data do not show that survival is affected by the presence or absence of clinical endocrinopathy. Interestingly, although complete macroscopic resection of hepatic metastases (R0/R1) has been undertaken more frequently, survival has not significantly differed among patients with complete or incomplete hepatic resection of metastatic NET, provided cytoreduction exceeds 90% of the estimated hepatic cancer volume (Que et al, 1995; Sartori et al, 2005). Significant improvement in quality of life with prolonged survival also has been confirmed for patients undergoing adequate (>90%) cytoreduction (Knox et al, 2004). These data suggest that hepatic resection of metastatic NET is safe and clinically effective, and overall operative survival is nearly double that of patients with unresected metastases. Few other factors related to the primary NET, metastatic disease, or patients appear to correlate with survival.
A major challenge is providing treatment for bilobar synchronous hepatic metastases, which are relatively common. Although one-step surgery may be feasible, it might require right portal vein embolization (see Chapter 93A, Chapter 93B ) to enhance the size of the future liver remnant. Compared with two-step surgical procedures that include resection of the primary and clearance of left liver, followed by right portal vein occlusion and a second step consisting of right or extended right hepatectomy, it seems that with or without preoperative portal vein embolization, one-step surgery is associated with a higher rate of R2 resection and more postoperative complications (Elias et al, 2003; Kianmanesh et al, 2008; Steinmuller et al, 2008). This might in part be due to preoperative intensive selection of patients in two-step procedures and dissociation of major liver and abdominal surgery; however, compared with liver transplantation, the two-step procedures represent a valid alternative by pushing the limit of respectability in type III patients, especially those with bilobar, synchronous liver metastases (Kianmanesh et al, 2008; Steinmuller et al, 2008).
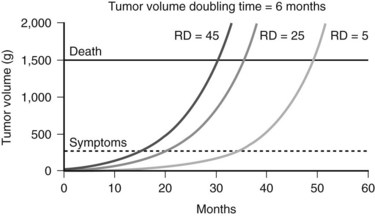
Complete resection remains the goal of cytoreductive hepatic resection, because both progression rate and median time to clinical recurrence are significantly reduced. The theoretic impact of minimizing residual metastatic NET in the liver on outcome is depicted in Figure 81B.3. Resection of more than 90% of the volume of hepatic metastases can result in significantly different residual cancer volumes based on variations of the incident metastatic volume. Figure 81B.3 shows the projected outcomes of three different residual tumor volumes on symptom recurrence and survival, assuming a greater than 90% resection and a cancer doubling time of 6 months. Both time to recurrence of symptoms and survival are related to residual metastatic cancer volume. The clinical impact of cytoreductive hepatic resection is not more than 90% resection of metastatic NET in the liver but the minimization of residual metastatic volume, that is, not resected volume but rather residual liver volume.
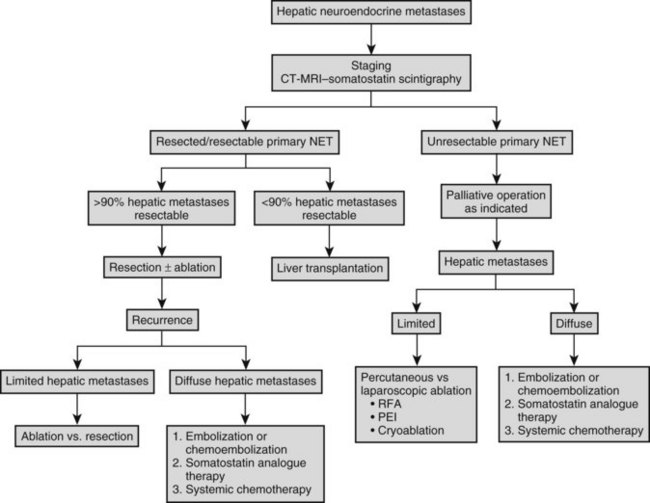
The overall frequency of recurrence or progression after hepatic resection is approximately 80% at 5 years. Intrahepatic progression of residual metastases after R1 or R2 resection or recurrence after R0 resection dictates subsequent liver-directed therapy, unless the risk of liver failure or extrahepatic disease spread override this issue. Although cure of patients with metastatic NET to the liver is infrequent, prolonged palliation is possible. Patterns of intrahepatic recurrence have not been well studied, but intrahepatic recurrence is typically multicentric in our experience. The extent and distribution of hepatic recurrence dictates the choice of therapy. For solitary recurrences, either resection or ablation is appropriate. Given that serial imaging usually identifies small recurrences after hepatic resection, percutaneous ablative approaches are preferable, because morbidity associated with percutaneous RFA is less than that after repeat resection, which is advised for lesions in sites that preclude safe RFA. Sequential ablation or resection is undertaken as recurrence is recognized, until precluded by extent of recurrence within the liver. Metastatic NET that precludes ablation or resection is treated by embolization or chemoembolization, with or without systemic chemotherapy in the absence of extrahepatic disease and with chemotherapy in the presence of extrahepatic disease. A schema for management of neuroendocrine metastases to the liver is outlined in Figure 81B.4.
Hepatic Transplantation for Neuroendocrine Metastases (See Chapters 97A and 97E)
Orthotopic liver transplantation (OLT) has been frequently employed for the treatment of metastatic NET (Table 81B.2). The rationale for OLT is similar to that for resection, with the caveat that adequate cytoreduction by resection is precluded by extensive intrahepatic disease and the absence of extrahepatic metastases. OLT during the time period of intrahepatic disease may be curative or at least significantly palliative. Unlike resection, OLT addresses all hepatic metastases and should provide similar, if not greater, duration of palliation of symptoms and survival. The attractiveness of R0 resection afforded by OLT and the high recurrence rate of NET associated with resection has fostered ongoing evaluation of OLT for metastatic NET (Mazzaferro et al, 2007).
Table 81B.2 Hepatic Transplantation for Metastatic Neuroendocrine Tumors
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


