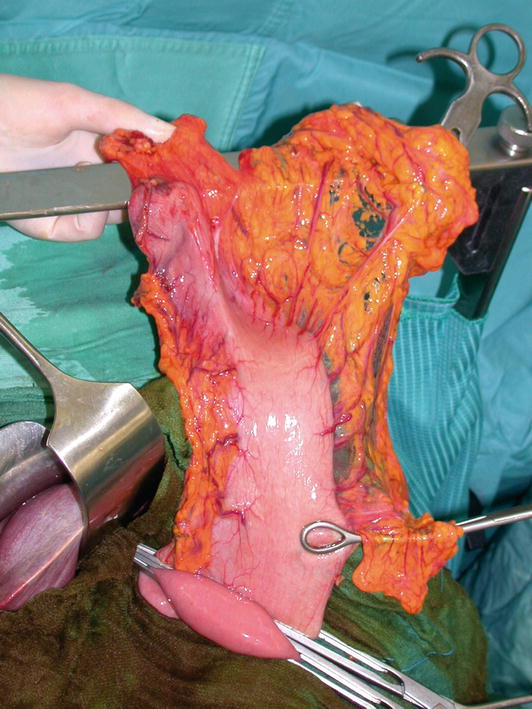
Fig. 4.1
Complete removal of lymphatic and adipose tissue of the proximal portion of the lesser curvature up to the right wall of the cardia exposes the medial wall of the stomach and the esophagogastric junction, ensuring optimal exposure and safe closure of the medial portion of the gastric stump
Fig. 4.2
The right paracardial (station 1) and proximal lymphatic and adipose tissue of the lesser curvature (station 3) is thus removed, dissected, and sent for definitive histology. The arteriovenous branches of the left gastric pedicle, which penetrate the gastric wall, also need to be ligated close to the gastric wall
4.3 Preservation of Gastric Stump Vascularity
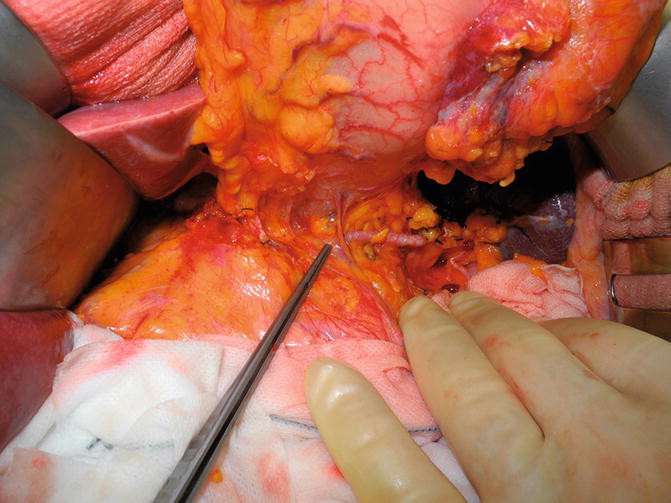
Fig. 4.3
After identification of the transection point on the greater curvature, the gastric wall is dissected at this level, carefully preserving two or more short gastric vessels and the posterior gastric artery to ensure viability and trophism of the gastric stump
4.4 Preparation of the Jejunal Loop and Roux Limb Transposition to the Supramesocolic Compartment

Fig. 4.4
With the transverse colon gently retracted, the second jejunal loop and the associated mesentery are spread to examine the anatomy of its arterial arcades by transillumination
Fig. 4.5
The arcades are then divided nearly up to the base of the mesentery, to mobilize the jejunum and gain tension-free access to the gastric stump
Fig. 4.6
The resection site on the jejunum is then identified, and the jejunum is closed with a TA 30 linear stapler; after placement of a non-crushing intestinal clamp, the afferent portion is also resected with a traditional blade and remains open. The stapled efferent portion is oversewn with interrupted slowly absorbable 3-0 sutures. With the transverse colon still gently retracted, an avascular area in its left inferior paramedian portion is identified by transillumination and incised to allow transposition of the efferent jejunal limb to the supramesocolic compartment through the transverse mesocolon
4.5 Placement of the Haberer Intestinal and Stomach Clamp
Fig. 4.7
The gastric tool of the Haberer intestinal and stomach clamp is applied to the gastric fundus at an adequate distance between the proximal tumor pole and resection line, considering that the anastomosis will be executed ca. 2 cm below the clamp. The nasogastric tube is withdrawn before closing the clamp, to avoid its entrapment
Fig. 4.8
The gastric tool of the Haberer clamp should be applied to the gastric fundus at an obtuse angle (120–130°) with respect to the lesser curvature. In this way, the transection line affords both macroscopically correct margins and removal of antral G cells (thus avoiding retained antrum syndrome)
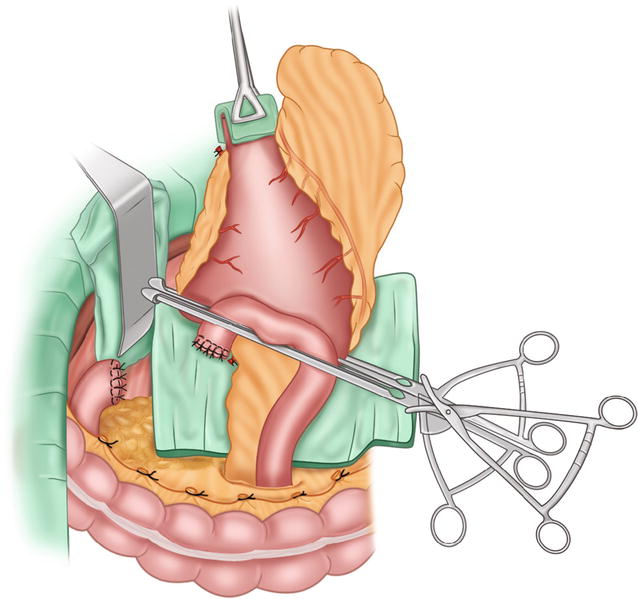
Figs. 4.9 and 4.10
With the stomach elevated and retracted upward, to expose its posterior wall which is held in slight tension, the first assistant raises the previously prepared closed Roux limb with two forceps, while the surgeon gently tightens the jejunal tool of the clamp at the level of the mesenteric edge. The gastric and jejunal wall are approximated on the lateral side of the greater curvature. The gastric and jejunal clamps are then brought close together and blocked with the third clamp. The latter is locked when the gastric and the jejunal wall are approximated on the lateral side of the greater curvature. Three laparotomy pads, one behind the stomach, another in front of the Roux limb, and the third above the three clamps, are applied prior to execution of the anastomosis, to prevent contamination of the operating field and trapping of the suture threads in the clamp jaws
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


