Figs. 3.1 and 3.2
The inferior (pars flaccida) and superior (pars condensa) portions of the lesser omentum are resected close to the liver, so that they can be removed en bloc with the stomach. If the lesser omentum is divided up to the right crus of the diaphragm and the right esophageal wall, the lymphatic and adipose tissue of the lesser curvature and the right paracardial lymph nodes will remain attached to the stomach
3.2 Resection of the Gastrosplenic Ligament

Figs. 3.3 and 3.4
On the side of the greater curvature, the gastrosplenic ligament is identified and resected, proceeding from low to high, carefully ligating its 4–6 short gastric vessels or dividing them with the ultrasonic or radiofrequency scalpel.
After ligation of the first and second short gastric vessels, the spleen is definitively freed from the stomach, and access is gained to the left paracardial region and crus of the diaphragm.
Only the tumor’s close relationship to the spleen or the presence of multiple, macroscopically enlarged splenic hilar lymph nodes warrants splenectomy en bloc with the gastric specimen
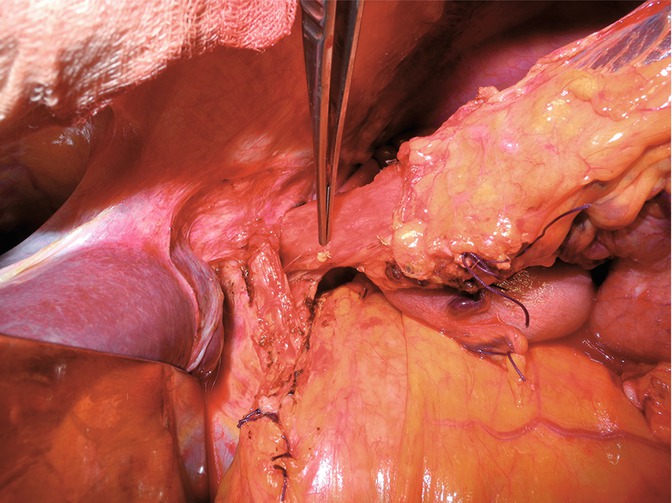
3.3 Division of the Phrenoesophageal Membrane and Vagus Nerves
Figs. 3.5, 3.6, and 3.7
Section of the left triangular and coronary ligaments and right dislocation of the left leaver segments allow excellent exposure of the esophago-cardial region. Resection of the Lymer-Bertelli phreno-esophageal membrane releases the anterior esophageal wall and allows complete dissection of the intra-abdominal esophagus
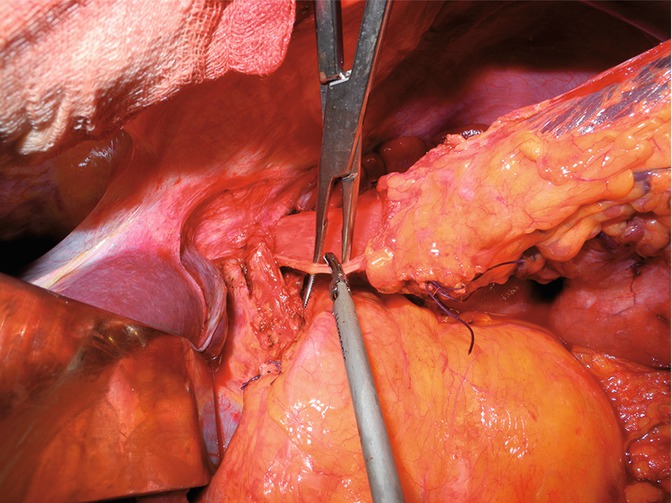
Figs. 3.8 and 3.9
Division of the two vagus nerves, which are easily identified because they are strung longitudinally at the level of the external portion of the esophageal wall, allows further mobilization of the intra-abdominal esophagus. Their division after dissection results in immediate collapse or greater mobility of the intra-abdominal esophagus
3.4 Rake Clamp Positioning, Purse-String Suture, Esophageal Resection, and Stapler Anvil in the Distal Esophagus
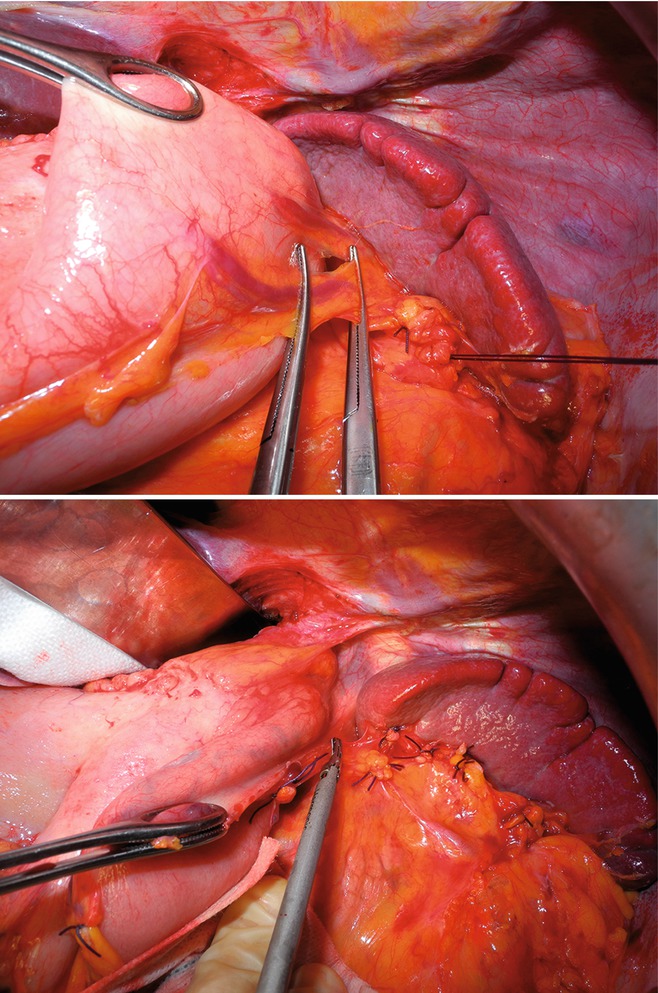
Fig. 3.10
A rake clamp is positioned at the center of the intra-abdominal esophagus on macroscopically healthy tissue, 1–2 cm upstream of the cardia, carefully avoiding trapping the nasogastric tube. Two straight needles are inserted through the rake clamp jaws to execute a purse-string suture in the distal esophagus with nonabsorbable monofilament suture 2-0
Figs. 3.11 and 3.12
The surgeon cuts the distal esophagus with curved scissors close to the rake clamp, thus freeing the specimen, which consists of the whole stomach, the omentum, and all first-level perigastric lymph nodes (stations 1–6). The specimen is submitted for intraoperative consultation to establish the tumor’s distance from the proximal and distal margins and exclude microscopic positivity
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


