Chapter 54 Management of acute pancreatitis and complications
Overview
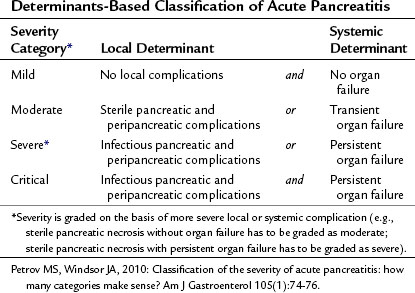
The severity of acute pancreatitis (AP) varies from mild uncomplicated disease to critical disease associated with both local and systemic complications (see Chapters 52 and 53). It is important to determine the severity of acute pancreatitis in the individual patient for triage, treatment, and prognosis. Since 1992, when the International Symposium on Acute Pancreatitis in Atlanta published its consensus, it has become customary to define the severity of acute pancreatitis as either mild or severe (Bradley, 1993). Acute pancreatitis is severe when it is associated with local or systemic complications. Although the Atlanta classification was a significant advance, it is now accepted that the dichotomous approach fails to capture clinically relevant categories of patients (Petrov & Windsor, 2010). For instance, it does not allow for discrimination among patients with transient and persistent organ failure, those with sterile and infectious local complications, and those with either local or systemic complications.
A large body of evidence now demonstrates that the two key determinants of severity in acute pancreatitis are organ failure—absent, transient, or persistent—and pancreatic complications—absent, noninfectious, or infectious. Determinants-based classification of the severity of acute pancreatitis composed of four categories (Table 54.1) appears to be more useful for the clinical assessment of severity in individual patients and for comparing groups of patients (Petrov & Windsor, 2010). The distinct advantages of this new classification is that it uses widely accepted and unambiguous terms, it can be applied in both early and late phases of acute pancreatitis, it can facilitate communication between treating physicians, and it promotes standardization for management of acute pancreatitis (Petrov et al, 2010).
Although many aspects of the management of acute pancreatitis remain controversial, significant overall progress has been made during the last few decades, evidenced by a reduction in morbidity and mortality rates (Lowenfels et al, 2009; Banks & Freeman, 2006). The improved outcomes have not been due to any treatments based on specific, critical pathophysiology. A wide range of drugs has been evaluated in randomized controlled trials (RCTs) and have proved ineffective in the treatment of acute pancreatitis. These include aprotinin, atropine, calcitonin, fresh frozen plasma, glucagon, gabexate, glucocorticoids, lexipafant, nonsteroidal antiinflammataory drugs (NSAIDs), and octreotide. The overall improvement in outcome for patients with acute pancreatitis has been due to a combination of factors that include improvements in intensive care medicine, imaging techniques, severity prediction, and selection of patients for endoscopic retrograde cholangiopancreatography (ERCP) and surgery.
General Management
Pain Management
Pain is the cardinal symptom of acute pancreatitis, and its relief is a clinical priority. The strategy in patients with acute pancreatitis, as for all acute pain, is the staged use of analgesics. Although some debate still surrounds step-up and step-down approaches, it is best practice to use NSAIDs for the management of mild pain (Pezzilli et al, 2007). The potential risk of bleeding as a result of the antiplatelet effect of NSAIDS has not been an issue in practice. For patients with moderate and severe pain, and for those for whom NSAIDs are inadequate, the second step is to use a weak opioid; the third step is to use a strong opioid.
Although experimental findings show that morphine can induce spasm of the sphincter of Oddi and exacerbate the severity of acute pancreatitis, it is worth noting that the avoidance of morphine as an analgesic has not been supported by clinical studies (Economou & Ward-McQuaid, 1971). A comprehensive review of the literature shows that all opiates increase the pressure in the sphincter of Oddi but that physiologic effect is of marginal clinical relevance (Thompson, 2001).
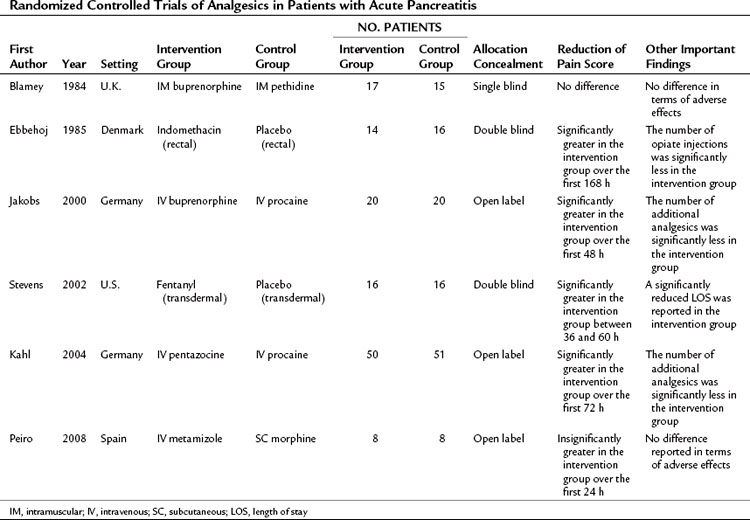
Different analgesics have been compared in patients with acute pancreatitis, and the six published RCTs are summarized in Table 54.2 (Blamey et al, 1984; Ebbehoj et al, 1985; Jakobs et al, 2000; Kahl et al, 2004; Peiro et al, 2008; Stevens et al, 2002). These trials had a different study design, evaluated different analgesics, and had small sample sizes; only three of the trials were double-blinded. From these studies it can be said that no credible clinical evidence supports avoiding the use of morphine in treating the pain associated with acute pancreatitis; however, the NSAID of choice is metamizole (2 g/8 h IV), and the opioid of choice is buprenorphine (0.3 g/4 h IV). There is no evidence to support the use of parenterally administered local anesthetics such as procaine in the management of pain associated with acute pancreatitis. However, the lack of high-quality evidence means that the choice of analgesic and the strategy for administration remain uncertain. No recent guidelines relating to the management of acute pancreatitis provide a specific recommendation regarding pain management (Loveday et al, 2010).
Fluid Resuscitation
Acute pancreatitis can be associated with substantial third-space fluid losses, and the resultant hypovolemia that impairs the microcirculation of the pancreas is a major determinant of pancreatic necrosis. The reflex splanchnic vasoconstriction in response to hypovolemia may compound pancreatic hypoperfusion and further predispose to ischemia. Fluid resuscitation is one of the most important aspects of the early management of acute pancreatitis (Gardner et al, 2008; Talukdar & Vege, 2009) and is the intervention most likely to improve outcome. No high-level evidence describes the optimal resuscitation fluid, required fluid rate, or best marker to guide resuscitation and indicate its adequacy (Banks & Freeman, 2006; Pandol et al, 2007). It is not even known whether colloids or crystalloids are more effective in improving pancreatic microcirculation and outcome. The initial goal of fluid resuscitation is to restore circulating blood volume (euvolemia), with the aim of normalizing heart rate, blood pressure, central venous pressure, and urine output, even though these do not reflect the adequacy of pancreatic and splanchnic perfusion (Flint & Windsor, 2003). In general, urine output should be restored at greater than 0.5 mL/h/kg body weight, and the central venous pressure should be restored to between 8 and 12 cm H2O. Swan-Ganz monitoring can be helpful in hemodynamically unstable patients, and some evidence shows that as an independent risk factor of pancreatitis severity and a marker of hydrations status, hematocrit might be useful with fluid resuscitation (Pitchumoni et al, 2005; Wu et al, 2009). Adequate fluid resuscitation is likely when the hematocrit is restored to between 30% and 35%. A number of other approaches to guide resuscitation offer promise but have not become established in clinical practice. An example is the use of intramucosal pH (pHi) derived by nasogastric tonometry (Juvonen et al, 2000a; van Haren et al, 2007), which is predictive of severity and reflects the adequacy of perfusion in the splanchnic circulation.
Antibiotics
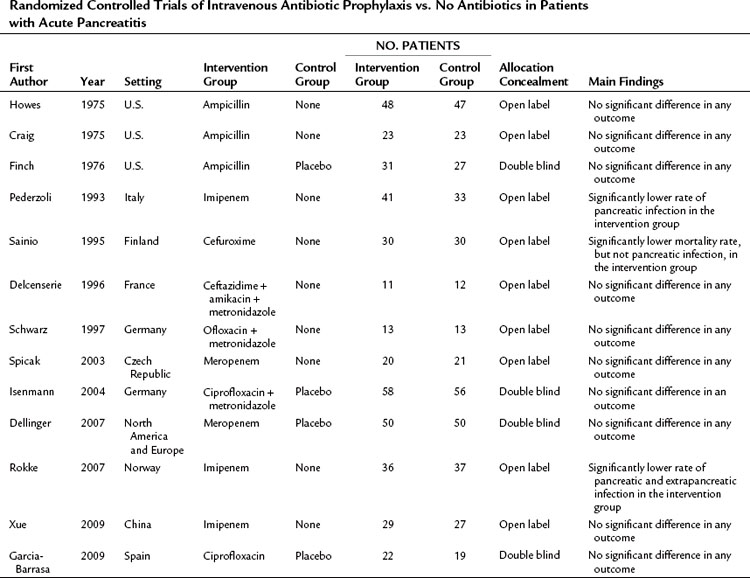
Although the use of broad-spectrum antibiotics to treat the established infection in acute pancreatitis is a well-established practice, the use of prophylactic antibiotics has been controversial for decades. Three RCTs in the 1970s failed to demonstrate a beneficial effect of antibiotic prophylaxis, probably because of a small sample size, inappropriate selection of antibiotics—such as ampicillin, which does not sufficiently penetrate the pancreas—and inclusion of patients with mild pancreatitis (Table 54.3; Craig et al, 1975; Finch et al, 1976; Howes et al, 1975). Between 1993 and 2009, several randomized, controlled, open-label trials were published evaluating the efficacy of prophylactic antibiotic treatment in patients with severe acute pancreatitis (Delcenserie et al, 1996; Pederzoli et al, 1993; Rokke et al, 2007; Sainio et al, 1995; Schwarz et al, 1997; Spicak et al, 2003; Xue et al, 2009). The results of these trials were conflicting. Although some RCTs demonstrated a significant reduction of infectious complications and mortality with the use of prophylactic antibiotics, others failed to do so (see Table 54.3). Only three double-blind, placebo-controlled RCTs were published between 2004 and 2009, and all of them were unable to show a beneficial effect of antibiotic prophylaxis regarding infectious pancreatic complications, the need for surgery, and mortality (Dellinger et al, 2007; Garcia-Barrasa et al, 2009; Isenmann et al, 2004). This is in line with the findings of a meta-analysis that showed an inverse relationship between methodologic quality of the studies and impact of antibiotic prophylaxis on mortality (de Vries et al, 2007).
Table 54.3 Randomized Controlled Trials of Intravenous Antibiotic Prophylaxis vs. No Antibiotics in Patients with Acute Pancreatitis
Several attempts have been made to statistically aggregate data on the use of prophylactic antibiotics in acute pancreatitis. Although only two new RCTs were published from 2006 through 2007, it is notable that seven of the 10 meta-analyses were published within this period (Petrov, 2008). Thirteen RCTs were included in these seven meta-analyses. Because of different inclusion criteria and various meta-analysis techniques used, concordance is lacking, and they provide contradictory recommendations regarding the role of prophylactic antibiotics in reducing the risk of pancreatic infectious complications. Overall, it appears that the most recent studies do not support the use of prophylactic antibiotics to reduce the frequency of pancreatic infectious complications, surgical intervention, and death in patients with acute pancreatitis. Therefore routine broad-spectrum prophylactic antibiotics in patients with severe acute pancreatitis cannot be recommended on the basis of current evidence.
Nutritional Management
Severe acute pancreatitis is associated with a cytokine-mediated systematic inflammatory response and a hypercatabolic state (Windsor & Hammodat, 2000; see Chapter 10). The adverse consequences of this include protein-calorie malnutrition, expansion of the extracellular fluid compartment, and immune suppression. A meta-analysis of RCTs showed that nutritional support, both enteral and parenteral, significantly reduced risk of mortality in patients with acute pancreatitis compared with no nutritional support (Petrov et al, 2008c). Nutritional support is thus an essential part of the management of patients with severe acute pancreatitis (Banks & Freeman, 2006; Pandol et al, 2007).
Type of Feeding
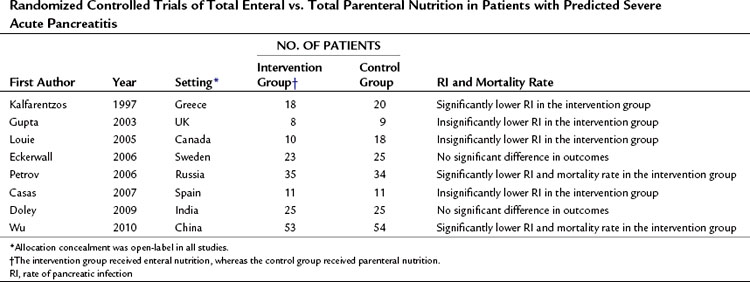
A number of RCTs compared total PN and total EN in the management of predicted severe AP (Table 54.4; Casas et al, 2007; Doley et al, 2009; Eckerwall et al, 2006; Gupta et al, 2003; Kalfarentzos et al, 1997; Louie et al, 2005; Petrov et al, 2006; Wu et al, 2010). A meta-analysis of high-quality RCTs has shown a significant twofold reduction in the risk of total and pancreatic infectious complications and a 2.5-fold reduction in the risk of death in patients receiving total EN (Petrov et al, 2008f). The basis for the clinical benefits of EN over PN remain unclear, although EN may prevent or attenuate mucosal barrier failure and bacterial translocation (Windsor & Hammodat, 2000). Intestinal permeability studies are a surrogate marker for clinically relevant events and provide conflicting results. Three clinical studies showed increased intestinal permeability to both micromolecules and macromolecules in patients with severe acute pancreatitis when compared with mild acute pancreatitis and healthy volunteers (Ammori et al, 1999; Juvonen et al, 2000b; Nagpal et al, 2006). But an early RCT from the United Kingdom (Powell et al, 2000) in which patients with predicted severe AP were randomized to receive either EN or no artificial nutritional support showed significantly increased intestinal permeability by day 4 in patients allocated to the EN group. Similarly, a recent RCT from Sweden comparing nasogastric EN and PN in patients with predicted severe acute pancreatitis demonstrated impaired gut permeability on day 3 in the EN group (Eckerwall et al, 2006). This difference might be explained by the inclusion of a considerable number of patients with mild AP in whom intestinal permeability is unlikely to change (Petrov et al, 2008f).
Route of Enteral Feeding
Nasogastric (NG) tube insertion may be more practical than nasojejunal (NJ), as the latter often requires endoscopy or radiology expertise, the transfer of patients within the hospital, and a delay in starting feeding. However, NJ EN has been preferred to NG EN because of a fear about pancreatic stimulation. Pancreatic response to feeding was studied in human volunteers, and it was shown that all forms of EN, with the exception of NJ feeding, stimulate pancreatic secretion (O’Keefe et al, 2003). By contrast, a study in patients with acute pancreatitis showed a significantly lower rate of secretion of trypsin, amylase, and lipase in comparison with healthy subjects (O’Keefe et al, 2005). Moreover, it was shown that the greater the severity of acute pancreatitis, the greater the reduction in pancreatic enzyme secretion as a response to duodenal feeding, probably reflecting greater injury of acinar cell mass. The possible clinical implication of these findings is that NG EN may not aggravate the course of acute pancreatitis, as was previously suggested.
Two RCTs have compared NG EN with NJ EN in patients with severe acute pancreatitis (Eatock et al, 2005; Kumar et al, 2006). These studies demonstrated the feasibility, safety, and tolerance of NG EN, but a meta-analysis did not demonstrate a statistically significant reduction in risk of death (Petrov et al, 2008b). Before NG EN can be considered the standard of care in the nutritional support of patients with AP, a well-designed and adequately powered RCT comparing mortality and morbidity of NG EN and NJ EN is required. A practical compromise is to start EN through an NG tube after the patient has been resuscitated and for the tube to be advanced when endoscopic or radiologic assistance is available.
Type of Enteral Feeding
The concept of “pancreatic rest” has also influenced decisions about the type and content of enteral feeding. The preferred formulations, elemental and semi-elemental formulas (Roberts, 2001; Petrov, 2007), did not require pancreatic enzymes for digestion and absorption. However, the major disadvantage of elemental and semi-elemental formulas is the cost, which is reportedly threefold to sevenfold higher than that of polymeric formulas. A recent meta-analysis of RCTs compared these two formula types in terms of feeding intolerance, infectious complications, and mortality and found that the use of polymeric over elemental and semi-elemental feedings did not result in reduced tolerance in patients with acute pancreatitis and appeared to reduce the risk of infectious complications and death (Petrov et al, 2009a). Thus the use of elemental and semi-elemental formulas confers no apparent advantage over relatively inexpensive polymeric formulas.
Because the gastrointestinal tract is the largest immune organ, containing approximately 65% of the immune tissue in the body, it has been considered that the use of immune-enhanced enteral formulations might increase the beneficial effects of EN in acute pancreatitis (Bengmark, 1999; Schloerb, 2001). Several trials were performed in different clinical settings, which suggested that immunonutrition might have the potential to modify the inflammatory response. The results of RCTs that compared the use of immune-enhanced and standard enteral formulas were statistically aggregated in several meta-analyses (Beale et al, 1999; Heyland et al, 2001; Heys et al, 1999). The most recent and comprehensive systematic review of 2419 patients from 22 RCTs (Heyland et al, 2001) found that the effect of immune-enhancing EN may depend on the subset of the analyzed patients. In particular, no effect of immunonutrition on the risk of infectious complications or death was reported within the subgroup of critically ill patients. At the same time, administration of a formula high in arginine in a combined group of critically ill and elective surgery patients was associated with a statistically significant reduction in infectious complications and a trend toward lower mortality rates in comparison with other immune-enhancing diets. A recent meta-analysis of RCTs in patients with acute pancreatitis did not show any clinical beneficial effect of immunonutrition when compared with standard EN (Petrov et al, 2008a).
Tolerance of Enteral Feeding
Dieticians generally agree on the caloric target in patients with acute pancreatitis: 30 kcal/kg and 1.5 g/kg of protein daily based on ideal body weight (Andersson et al, 2009; Olah & Romics, 2008). To ensure tolerance of EN, it is usually commenced at a low rate of 25 to 30 mL/h and increased incrementally over a day or more, until the desired caloric intake is reached. Despite this approach, EN can be associated with feeding intolerance in some patients with acute pancreatitis. Most commonly, the intolerance manifests as abdominal distension, delayed gastric emptying, gastroesophageal reflux, and diarrhea, all of which may develop in the presence of sepsis or with a significant clinical deterioration. In general, tolerance is achieved when EN is provided without development of one of these complications (Bankhead et al, 2009; Mallampalli et al, 2000). Various strategies to improve tolerance to EN require clinical studies, which are also needed to investigate markers of gut motility, absorption, and blood flow that can be easily applied at the bedside.
Timing of Enteral Feeding
The best time to start EN in patients with acute pancreatitis has never been studied. The indirect evidence in regard to this is derived from trials of EN versus PN only. Some authors have demonstrated clinical benefits of early enteral nutrition, but others have demonstrated the favorable effects of delayed enteral feeding (Petrov et al, 2009b). Early EN should help maintain gut integrity (enterocyte population) and function (motility) and reduce bacterial translocation and ileus. It should also help to achieve caloric targets more quickly. But early nutrition is not without risk, particularly in hemodynamically unstable patients and in those requiring inotropic support. These patients appear to be at an increased risk of nonocclusive mesenteric ischemia, and it is best to commence EN after adequate resuscitation.
Therapeutic Endoscopic Retrograde Cholangiopancreatography
Endoscopic retrograde cholangiopancreatography (ERCP) with endoscopic sphincterotomy (ES) has been promoted as a proven intervention in patients with acute biliary pancreatitis since the early 1990s (see Chapters 18 and 27). This was based on the findings of two RCTs, from the United Kingdom and Hong Kong, of early ERCP (within 24 to 48 hours of admission) with or without ES versus conservative treatment (Neoptolemos et al, 1988; Fan et al, 1993). Both trials demonstrated that early ERCP was associated with a reduction in complications, but not in mortality, and only in patients with predicted severe acute pancreatitis.
Some evidence suggests that the duration of biliary obstruction, rather than the predicted severity of acute pancreatitis, is the most important determinant of outcome (Acosta et al, 1997, 2006). This is probably due to concomitant cholangitis secondary to the obstruction and probably best explains the usefulness of ERCP in the context of acute biliary pancreatitis (Petrov, 2009). The first multicenter RCT to examine the role of ERCP in acute pancreatitis was designed to include only patients without evidence of biliary obstruction (Folsch & Neoptolemos, 2002). This German study did not find any benefit of early ERCP (within 72 h after onset of symptoms) over conservative treatment. The most recent RCT, from Argentina, found that early ERCP in patients with biliary obstruction, defined by laboratory and radiologic criteria, and without evidence of acute cholangitis conferred no benefit (Oria et al, 2007).
Two important meta-analyses were published in 2008. The first found that compared with conservative treatment, early ERCP in patients with both predicted mild and predicted severe acute pancreatitis did not decrease the incidence of local pancreatic complications or mortality rate (Petrov et al, 2008d). The second meta-analysis was designed to negate the confounding effect of acute cholangitis and demonstrated no benefit of early ERCP over conservative treatment in terms of complications and mortality in patients with predicted mild and predicted severe acute pancreatitis (Petrov et al, 2008e). The conclusion to be drawn from these studies is that early ERCP is indicated in patients with acute pancreatitis if acute cholangitis is evident (see Chapter 43) but not for those with just cholestasis (Petrov, 2009). Although cholestasis can reflect a persisting main bile duct stone, it might also be due to edema of the ampulla secondary to stone passage to the duodenum and may thus be expected to improve over the first few days of admission. Persistent cholestasis without cholangitis may require an ERCP but not usually in the acute setting.
Cholecystectomy
Recurrent attacks of gallstone pancreatitis carry a morbidity rate of up to 40% (Banks & Freeman, 2006), and an early laparoscopic cholecystectomy is widely advocated within the same hospital admission (see Chapter 30). The optimal timing of cholecystectomy has been controversial. The U.K. guidelines for the management of acute pancreatitis recommend that all patients with biliary pancreatitis undergo definitive management of gallstones during the same hospital admission (index cholecystectomy; Working Group, 2005). However, some surgeons have concerns that early surgery may be associated with an increase in operative difficulty and hence morbidity and conversion rate; therefore they advocate cholecystectomy after a period of 4 to 6 weeks to allow resolution of the inflammatory process (interval cholecystectomy; Green, 2008; Larson et al, 2006). These two approaches have been compared in several RCTs, which demonstrated no difference in complication rates between index and interval cholecystectomy; however, index cholecystectomy resulted in a significantly shorter length of hospital stay (Siddiqui et al, 2008). It is worth mentioning that patients with acute biliary pancreatitis were excluded from these trials. An adequately powered RCT of index versus interval cholecystectomy is needed to draw a firm conclusion about the optimal timing of cholecystectomy in patients with acute biliary pancreatitis.
Management of Systemic Complications
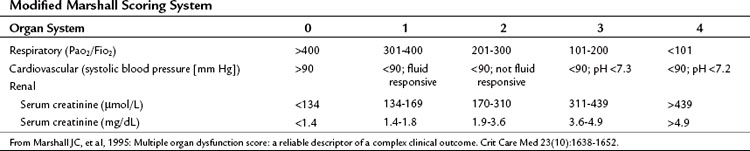
Most patients with acute pancreatitis have an initial sudden inflammatory respiratory syndrome response, others develop multiple organ dysfunction syndrome (MODS) in the first few days, and some develop MODS later in response to infectious complications (see Chapters 52 and 53). Patients with severe and critical acute pancreatitis are best managed in an intensive care environment to allow for optimal monitoring of fluid resuscitation and organ function and the early identification of life-threatening local or systemic complications. Systemic complications and organ failure are not an all-or-nothing phenomenon, rather a continuous spectrum exists between normal function of an organ system and its complete failure (Table 54.5; Marshall et al, 1995).
Some of the systemic complications of acute pancreatitis—coagulation abnormalities that may range from intravascular thrombosis to disseminated intravascular coagulation, metabolic disturbances (hyperlipidemia, hypocalcemia), liver failure, encephalopathy, and Purtscher retinopathy—are rare in clinical practice and beyond the scope of this chapter. In contrast, respiratory, cardiovascular, renal, and intestinal dysfunction are the most common systemic complications (Banks & Freeman, 2006; Pandol et al, 2007).
Respiratory failure is the most common systemic complication. The pathogenesis involves inflammatory cytokines released from the pancreas and the action of phospholipase A2 and other pancreatic catabolic enzymes on the lung. The clinical diagnosis of incipient respiratory failure is based on tachypnea and low oxygen saturation. A chest radiograph may confirm pleural effusions, pulmonary edema, and features of acute respiratory distress syndrome. Management is supportive, with oxygen supplementation and analgesia, and some patients will ultimately require endotracheal intubation and mechanical ventilation. Lung-protective ventilation strategies should be instituted, such as adequate positive end-expiratory pressures, permissive hypercapnia, and tidal volumes of 6 mL/kg ideal body weight (Nathens et al, 2004).
Patients with severe and critical acute pancreatitis can develop hypotension (arterial pressure <90 mm Hg) secondary to vasodilation and decreased systemic vascular resistance, and sometimes as a result of cardiotoxicity. Appropriate management consists of close hemodynamic monitoring, intravenous fluid resuscitation, and inotropic medications—dopamine at 2 to 10 µg/kg/min or dobutamine at 2 to 10 µg/kg/min—if indicated (Tonsi et al, 2009).
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Bile duct exploration and biliary-enteric anastomosis
Bile duct exploration and biliary-enteric anastomosis
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


