■ The patient should be secured to the operating room table with a chest strap, as extreme positioning is often necessary.
■ The right arm should be padded and tucked in a neutral position.
TECHNIQUES
ENTERING THE ABDOMEN AND INITIAL EXPOSURE
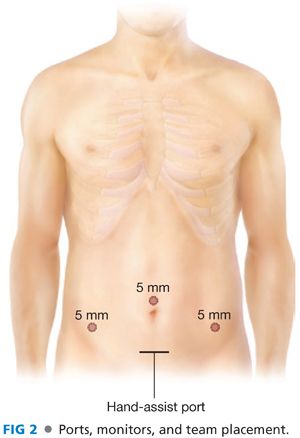
■ A Pfannenstiel or lower midline incision is created for hand-port placement (FIG 2). A 5-mm camera port is placed in the supraumbilical midline and 5-mm working ports are placed in the right lower quadrant and left lower quadrant positions.
■ In patients with prior abdominal surgery, laparoscopic access can be created by cut-down or Veress needle technique in a presumed safe location. This allows laparoscopic evaluation of abdominal wall adhesions, which can be lysed prior to creating the hand-port access. Alternatively, adhesions can be lysed in an open fashion through the hand-port incision; the surgeon’s ability to perform adhesiolysis in this fashion may be limited. Inability to lyse these adhesions can jeopardize the laparoscopic approach.
■ The patient is placed in steep Trendelenburg with the table tilted right side down.
■ The greater omentum is draped over the transverse colon and liver. The small bowel is retracted out of the pelvis and toward the right upper quadrant of the abdomen, exposing the sigmoid and left colon mesentery (FIG 3).
■ A laparotomy pad placed intraabdominally through the hand port aides in the retraction of the small bowel and in maintaining exposure. This also facilitates cleaning the scope without having to remove the scope from the abdomen. To reduce the chance of a retained pad, a hemostat is placed on the surgeon’s gown, signifying that a pad is in the belly. When the pad is removed (typically just prior to extraction), the hemostat is removed from the gown. If the surgeon goes to remove his or her gown with the hemostat still in place, the team is alerted that there may be a retained foreign body in the patient.

■ A 30-degree angled scope is used at the discretion of the surgeon. Angled scopes enable the surgeon to look over the horizon (particularly useful in splenic flexure takedown) and improves laparoscopic access to the field by allowing the scope to be held away from the dissection.
MESENTERIC DISSECTION, MEDIAL TO LATERAL
■ Commonly, the sigmoid and its mesentery are mobilized in order to permit extraction and the creation of a tension-free anastomosis. In cases where this degree of mobilization is not required, these steps may be omitted.
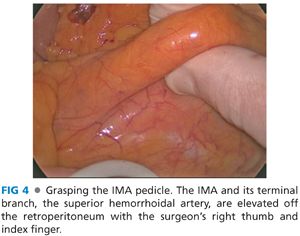
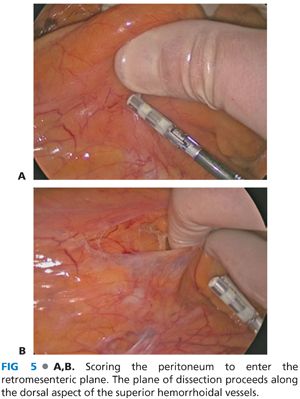
■ The surgeon stands at the patient’s right hip and the assistant stands at the right shoulder holding the camera at the umbilicus. The inferior mesenteric artery (IMA) pedicle is elevated with the surgeon’s right thumb and index finger (FIG 4) and is retracted toward the patient’s left hip. The surgeon uses an energy device through the right lower quadrant port to dissect dorsal to the IMA and its superior hemorrhoidal terminal branch (FIG 5). The aortic bifurcation and common iliac arteries are appreciated prior to starting the dissection. The peritoneum beneath the pedicle is scored to the level of the sacral promontory.
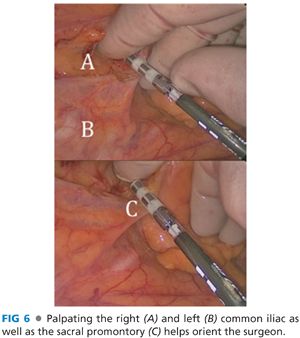
■ Palpating the right and left common iliac arteries located underneath the mesosigmoid and over the sacral promontory orients the surgeon (FIG 6).
■ Care is taken to preserve the hypogastric nerves located dorsal to the superior hemorrhoidal vessels.
■ The retromesenteric plane is developed by sweeping the retroperitoneum down (dorsally) and elevating the mesentery (FIG 6). The plane is developed laterally toward the side wall, superiorly over Gerota’s fascia and caudally toward the presacral space. As this is a relatively bloodless plane of dissection, bleeding is usually caused by injury to the overlaying mesentery or dissection into the floor of the space that is the retroperitoneum. Recognizing that you are not in the actual embryonic fusion plane allows you to adjust the dissection and reenter the correct plane.
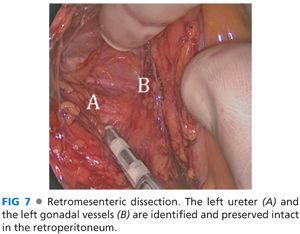
■ The left ureter and gonadal vessels are identified and preserved intact by sweeping these structures down into the retroperitoneum (FIG 7).
■ With the hand supinated within the retromesenteric space, a mesenteric window is created between the main sigmoidal artery and the left colic artery. The takeoff of the left colic artery is then divided with the energy device (FIG 8) while ensuring the left ureter is preserved intact in the retroperitoneum. Tumor localization should be confirmed (by intraoperative colonoscopy, if needed) prior to vessel ligation.
Related posts:
 End and Diverting Loop Ileostomies: Creation and Reversal
End and Diverting Loop Ileostomies: Creation and Reversal
 Parastomal Hernia
Parastomal Hernia
 Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
 Low Anterior Resection and Total Mesorectal Excision/Coloanal Anastomosis: Open Technique
Low Anterior Resection and Total Mesorectal Excision/Coloanal Anastomosis: Open Technique
 Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
 Total Abdominal Colectomy: Laparoscopic Technique
Total Abdominal Colectomy: Laparoscopic Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


