TECHNIQUES
SKIN INCISIONS
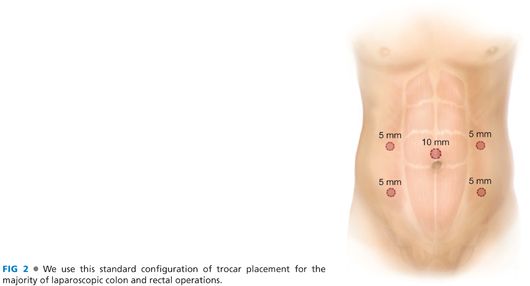
■ A Hasson technique is used to achieve access to the abdomen at the umbilicus.
■ Four 5-mm trocars are placed—two on either side of the abdomen lateral to the rectus with one hand breadth between the trocars. An optional fifth trocar can be placed in the suprapubic area if required for retraction. FIG 2 (trocars) shows the typical trocar placement.
LAPAROSCOPIC EXPLORATION
■ The abdomen is systematically explored in all four quadrants to look for metastatic disease and/or unexpected pathology.
■ Knowledge of the mesenteric anatomy is essential for a successful laparoscopic approach.
■ FIG 3 (colon anatomy) shows the colon with its major vascular pedicles. Also depicted is the gastrocolic trunk of Henle that can be a source of bleeding if not recognized during the dissection.
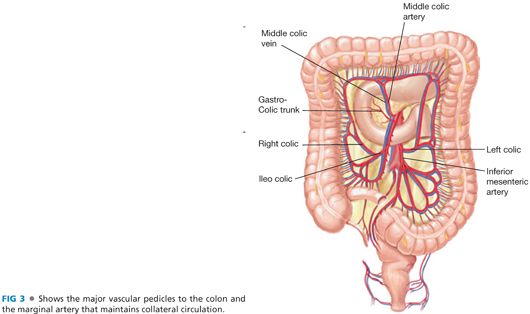
■ The right colic vessels commonly originate from the ileocolics (85%).
■ The middle colic arteries commonly have more than two branches (55%).
PEDICLE LIGATION
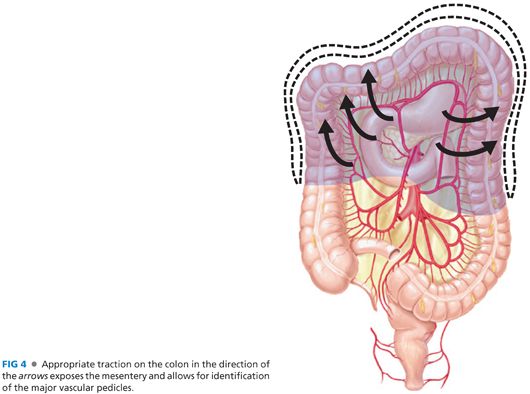
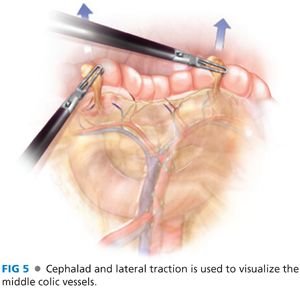
■ The ileocolic, middle colic, and left colic vessels are first identified (FIG 4). Identification of the vascular pedicles is facilitated by traction on the colon to tent the mesentery. Adequate exposure is achieved by grasping each flexure and retracting superiorly and laterally (FIG 5).
■ A window is created in the colon mesentery between the ileocolic and middle colic vessels. With appropriate traction and countertraction, the retromesenteric dissection is continued superiorly, medially, and laterally into the lesser sac (FIG 6).
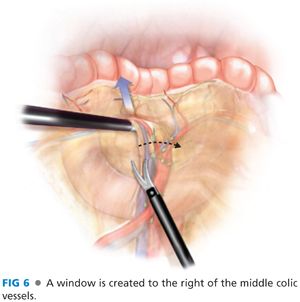
■ Care is taken to protect the duodenum, head of the pancreas, and the superior mesenteric artery (SMA) and vein during the dissection.
■ The middle colic vessels can be divided at the common trunk or divided individually after bifurcation (FIG 7). There is significant variation in the anatomy of the middle colic trunk.

■ Our practice is to use a bipolar vessel-sealing device to divide the pedicles, but clips and staplers are also options to divide the pedicles. It is important to ensure that the SMA and vein are protected and that sufficient cuff of the vascular pedicle is retained to control bleeding should the vessel sealers fail.
■ Strong anterior traction on the transverse colon mesentery optimizes middle colic dissection and decreases the likelihood of inadvertent injury to SMA.
RETROMESENTERIC DISSECTION
■ Right retromesenteric dissection
■ Laterally, the dissection is carried to the white line of Toldt and the hepatic flexure (FIG 8).

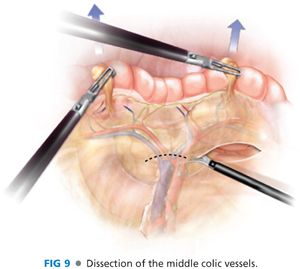
■ Medially, the dissection is carried to the root of the middle colic vessels and anterior to the head of the pancreas and the duodenum (FIG 9). The gastrocolic venous trunk is often encountered during this dissection and can be a source of bleeding if not recognized and controlled (FIG 10).

■ Superiorly, the dissection is carried cephalad to the transverse colon wall.
■ The remaining attachments to the liver are taken down (FIG 11).

■ Left retromesenteric dissection
■ A similar dissection is carried out on the left side, creating a window between the left colic and middle colic vessels (FIG 7).
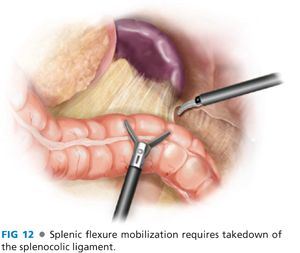
■ Laterally, the dissection is carried to the white line of Toldt and the splenic flexure of the colon (FIG 12).
■ Medially, the dissection is carried to the root of the middle colic vessels.
■ Superiorly, the dissection is carried to the inferior border of the pancreas and continued along the avascular plain between the left colon mesentery and the tail of the pancreas (FIG 13).

■
Related posts:
 End and Diverting Loop Ileostomies: Creation and Reversal
End and Diverting Loop Ileostomies: Creation and Reversal
 Parastomal Hernia
Parastomal Hernia
 Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
Surgical Management of Complicated Diverticulitis: Perforation and Colovesical Fistula
 Low Anterior Resection and Total Mesorectal Excision/Coloanal Anastomosis: Open Technique
Low Anterior Resection and Total Mesorectal Excision/Coloanal Anastomosis: Open Technique
 Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
Low Anterior Resection: Hand-Assisted Laparoscopic Surgery Technique
 Total Abdominal Colectomy: Laparoscopic Technique
Total Abdominal Colectomy: Laparoscopic Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


