Laparoscopic Total Mesorectal Excision
Hester Yui Shan Cheung
Michael Ka Wah Li
Chi Chiu Chung
Operating Room Setup and Position of the Patient
A dedicated team consisting of at least two experienced surgeons and one camera assistant is essential in practicing advanced laparoscopic procedures like laparoscopic total mesorectal excision (TME). These operations are ideally undertaken in an integrated endo-laparoscopic operating suite, where there is a universal plug and play system for various endoscopes and laparoscopes (1). The position of the patient and the surgical team are shown in Figure 34.1. Throughout the operation the patient is predominantly put in a 20 degree Trendelenburg position with right-side-down tilt, a position that helps clear the small bowel away from the lower abdomen and pelvis.
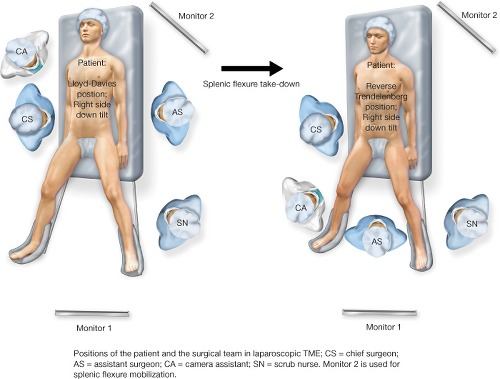 Figure 34.1 Positions of the patient and the surgical team in laparoscopic total mesorectal excision; CS = chief surgeon; AS = assistant surgeon; CA = camera assistant; SN = scrub nurse. Monitor 2 is used for splenic flexure mobilization. |
Recommended Instruments
(1) A 30 degree telescope
(2) Two atraumatic forceps for handling of bowel and soft tissues
(3) Two grasping forceps for holding cotton tapes
(4) Laparoscopic energy devices such as an ultrasonic dissection device or bipolar sealing and cutting devices
(5) Endo-staplers of various sizes and stapler height for bowel transection and vascular division
(6) Circular stapler for transanal anastomosis
(7) A sterile plastic zip-lock bag or an Alexis® wound retractors (Applied Medical, California, USA), used as parietal protective drape during specimen retrieval
Pneumoperitoneum and Insertion of Trocars
Pneumoperitoneum is first established by a subumbilical blunt trocar using an open technique. Other trocars are inserted under direct vision (Fig. 34.2).
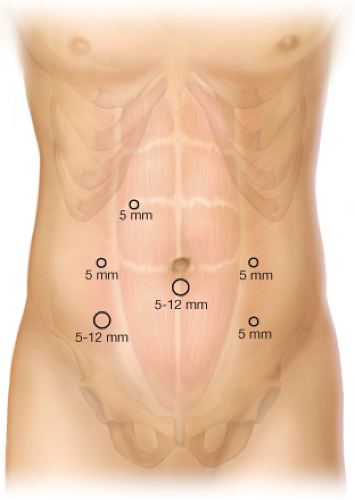 Figure 34.2 Port sites for laparoscopic total mesorectal excision or laparoscopic assisted abdominoperineal resection. An additional 5 mm port is created in the right upper quadrant if splenic flexure mobilization is necessary, as in the case of sphincter-saving resections. The chief surgeon and the camera assistant can use the subumbilical and the right iliac fossa ports interchangeably during splenic flexure mobilization. |
Exposure of the Pelvis
In female patients, for optimal exposure the uterus is first hitched up by passing sutures (00 Prolene on a straight needle) underneath the two fallopian tubes near the uterine cornua and tying them to the lower anterior abdominal wall (Fig. 34.3). The stitch should pass through the skin and be secured over a piece of gauze as a reminder to the surgeon to replace the uterus at the end of the procedure.
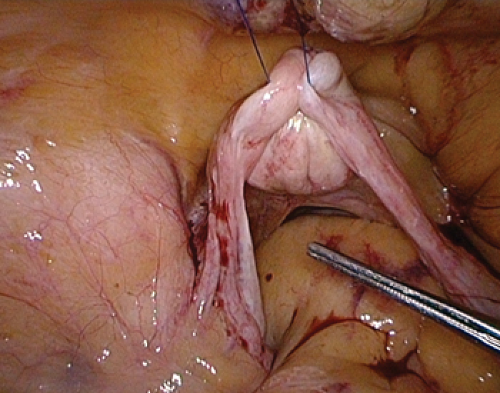 Figure 34.3 For optimal exposure of the pelvis, the uterus is hitched up to the lower anterior abdominal wall. |
Splenic Flexure Mobilization
Splenic flexure mobilization is required, especially when colonic J-pouch construction is intended.
We favor a medial-to-lateral approach in splenic flexure mobilization. The small bowel is kept in the right side of the abdomen by tilting the operating table to the right (right-side-down position). The inferior mesenteric vein is identified lateral to the duodenojejunal flexure, and is controlled and divided. Blunt dissection is then undertaken in the avascular plane between the mesentery of descending colon and the retroperitoneal fascia (Fig. 34.4). This dissection is laterally continued toward the splenic flexure




Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
