■ An exit site is identified in the skin of the left upper quadrant, several centimeters lateral from the midline. A stab incision is made at this level, and tonsil clamps are used to deliver the jejunostomy tube into the abdominal cavity.
Second Step—Choice of Tubes
■ The type of jejunostomy tube used can be as simple as a 10- or 12-French red rubber catheter or a silicone jejunostomy tube similar to those used in laparoscopic cases. Silicone tubes may have more longevity.4 Avoid using balloon-tipped catheters (i.e., Foley catheters) or, alternatively, ensure that the ability to inflate the balloon has been disabled to prevent future attempts at insufflating the balloon that could lead to subsequent bowel obstruction.
■ If using a red rubber catheter, the tip may be cut off, which allows for exchange over a wire should the tube become clogged. Additional side holes may also be cut at the distal end of the tube in order to improve flow through the catheter.
Third Step—Suturing Tube into the Bowel
■ The previously chosen site of proximal jejunum is delivered into the wound. The site of entry of the tube should be on the antimesenteric side of the jejunum. Once this is identified, a 3-0 silk is used to create a diamond-shaped purse-string suture. A small opening is made inside the purse-string suture with cautery, only large enough to allow for the tube to be inserted into the bowel.
■ The tube is placed into the bowel and advanced into the distal portion of the jejunum. The length of advancement into the jejunum should be long enough to prevent backflow of feeds into the proximal small intestine.
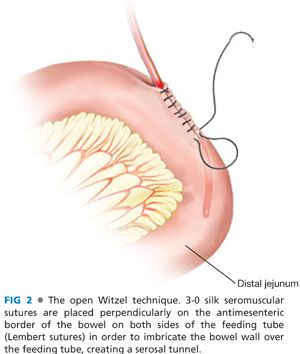
■ The purse-string suture is secured, and the tube is placed along the proximal bowel wall. The Witzel technique is then used to prevent extravasations of enteric feeds at the jejunostomy tube entrance site. In this technique, 3-0 silk seromuscular sutures are placed perpendicularly on the antimesenteric border of the bowel on both sides of the feeding tube (Lembert sutures) in order to imbricate the bowel wall over the feeding tube, creating a serosal tunnel (FIG 2). This should be approximately 2 to 3 cm in length and care should be taken to not narrow the lumen of the bowel or tube with these sutures. Care should also be taken to avoid perforating the feeding tube during the placement of these sutures, as this could lead to extravasation of the enteric feeds into the abdominal cavity.
Fourth Step—Suturing the Tube to the Abdominal Wall
■ The tube should then be secured with 3-0 silk seromuscular sutures to the abdominal wall parietal peritoneum in four quadrants around the exit point of the tube just proximal to the last Witzel suture. Care should be taken to avoid perforating the feeding tube during the placement of these sutures, as this could lead to extravasation of the enteric feeds into the abdominal cavity. One additional suture can be used to tack the jejunum to the abdominal wall distal to the tube entrance site to prevent kinking or volvulus of the jejunum around the tube site.
LAPAROSCOPIC JEJUNOSTOMY FEEDING TUBE PLACEMENT
First Step—Laparoscopic Port Placement
■ The abdomen may be entered either by a cut-down technique, by use of an insufflation needle followed by entry with an optical access trocar, or with an optical access trocar alone. One 5-mm port should be placed periumbilically and two additional 5-mm ports should be placed in a triangulated fashion to allow for manipulation of the jejunum; these should be placed under direct visualization to prevent bowel injury. These are traditionally placed in the right upper and left lower quadrants.
Second Step—Identification of the Ligament of Treitz
■ The patient is placed in a Trendelenburg position and is rotated to the right side in order to facilitate identification of the ligament of Treitz.
■ The transverse colon is elevated with an atraumatic grasper to identify the ligament of Treitz, located at the base of the transverse mesocolon and to the left of the fourth portion of the duodenum (FIG 1). A segment of jejunum approximately 15 to 20 cm distal from the ligament that will easily allow the jejunum to reach the abdominal wall without tension is identified.
Third Step—Placing the Tube in the Jejunum
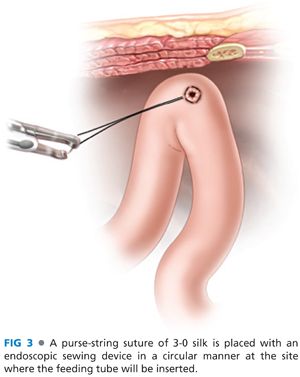
■ A purse-string suture of 3-0 silk can be placed with a laparoscopic needle driver or with an endoscopic sewing device in a circular manner, in the same fashion as performed in open cases (FIG 3). Using electrocautery, make an opening in the small bowel and deliver the feeding tube through the opening and into the distal jejunum. The purse-string suture is tied intracorporeally.
■ Lembert sutures are placed to create a Witzel serosal tunnel around the feeding tube. The jejunostomy tube is then tacked to the anterior abdominal wall with a four-quadrant suture placed intracorporeally proximally to the Witzel tunnel.
■
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


