Hand-Assisted
David A. Margolin
Laparoscopic total abdominal colectomy is one of the more challenging laparoscopic colon procedures (LAP) as the surgeon is asked to work in all four quadrants of the abdomen. The use of hand-assisted laparoscopic (HAL) techniques has been shown not only to facilitate the technical aspects of the procedure by restoring some tactile sensation, but also to decrease the operative time. In essence, it makes laparoscopic procedures “more like open surgery.” The indications for the procedure are the same whether performed open, laparoscopic, or hand assisted. However, it is up to the surgeon to determine if the patient is a candidate for minimally invasive surgery. They need to take into account the patient’s overall comorbidities as well as surgical history. While multiple previous abdominal operations are not an absolute contraindication for LAP or HAL, the individual surgeon’s level of comfort and experience with the planned procedure plays a large role.
Preoperative Preparation
Standard mechanical bowel preparation is not mandatory. However, it is the author’s preference, since it is easier to handle an empty colon. Our patients use a polyethylene glycol (PEG) preparation prior to surgery and maintained on clear liquids the day before surgery. We no longer use oral antibiotics prior to surgery but ensure that standard intravenous broad-spectrum antibiotics are given within 1 hour of skin incision. Since the patients will be in a modified lithotomy position for several hours deep vein prophylaxis is mandatory. We utilize both subcutaneous heparin and sequential compression stockings commencing immediately prior to surgery and continued after surgery. All patients have an informed consent that includes the potential for conversion to an open procedure.
Patient Positioning and Preparation
The patient is placed on a gel pad to prevent slippage. After induction of general anesthesia an orogastric tube and indwelling urinary bladder catheter are placed. The patient is placed in a modified lithotomy position using Yellow Fin Stirrups™ (Allen Medical, Batesville, IN) with the thighs even with the hips and all potential pressure points appropriately padded. Care is taken to ensure that there is no pressure on the peroneal nerves and that the patient’s knees are in line with contralateral shoulder. Both arms are tucked in the adducted position to facilitate securing the patients for the extremes of positioning used during laparoscopy. The patient is then secured to the table, with tape across the chest and the forehead to limit neck movement. Rectal irrigation is performed. After that the skin is prepped with a 2% chlorhexidine-based solution and draped in a standard fashion. Prior to draping the table is rotated in all directions to assure that the patient is stable.
Instrument/Monitor Positioning
Two monitors are utilized during the procedure. One is on the patient’s right side at the level of the shoulder. The other monitor is placed on the patient’s left side at the level of the hip. At our institution the monitors are mounted on booms from the ceiling allowing easy repositioning for optimal visualization. Because of the configuration of our operating rooms the insufflation tubing, suction tubing, cautery power cord, laparoscopy camera wiring, and a laparoscope light cord are brought off the patient’s left side at the foot of the table. We routinely use a 10-mm laparoscope with a 30-degree lens. However, with the increased availability of high-definition cameras and monitors a 5-mm laparoscope may be an acceptable alternative.
Port Selection and Placement
Prior to placing any ports the outline of the hand-assist device is marked on the patient’s abdomen. We use the Applied Medical GelPort® (Applied Medical, Ranch Santa Margarita, CA). By tracing the outline of the device we ensure that all of our ports are outside the outline to function throughout the procedure. We place the inferior edge of the device 2–3 cm from the pubic symphysis in the midline. Once this marking is done, we use a modified Hasson technique to enter the abdomen above the umbilicus and obtain pneumoperitoneum. A vertical skin incision is made with a scalpel followed by dissection down to the linea alba. A Kocher clamp is used to elevate the fascia in the midline at the level of the umbilical stump and the linea alba is then incised. S-shaped retractors are helpful in exposing the midline. Entry into the peritoneal cavity is accomplished sharply. Once entry into the peritoneal cavity is obtained a 10-mm blunt-tip balloon trocar is placed and inflated. A total of four additional ports are used. We use two 5-mm ports in the left and right upper quadrants and a 5-mm port in the left lower quadrant. We will often place a 12-mm port in the right lower quadrant, as this will allow placement of an endoscopic stapler if necessary; the hand port is placed later in the procedure (Fig. 23.1).
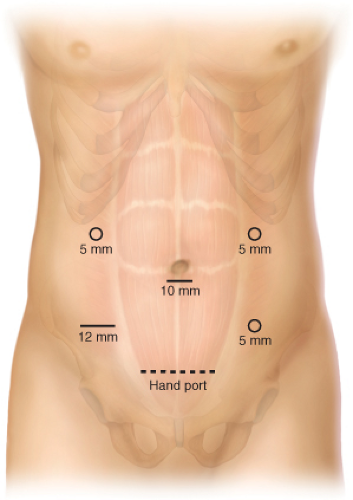 Figure 23.1 Laparoscopic port sites and hand port placement. |
Mobilization and Transection
After establishing pneumoperitoneum and placing the necessary ports the abdominal cavity is laparoscopically explored. The patient is then placed in the Trendelenburg position and is rotated to their left. We initially begin with right colon mobilization prior to placement of the hand port. Unlike other authors, we find that placing the hand port prior to mobilizing the right colon actually slows down the operation. First, the
ileocolic artery is grasped and elevated, and the avascular plane on either side is dissected free to allow clear visualization of the duodenum. The vessels are then ligated and divided using a vessel-sealing device such as the Ethicon EnSeal® (Ethicon Endosurgery, Cincinnati, OH) although the choice of the alternate energy source is up to the surgeons’ discretion. Care is taken at this point to sweep the duodenum medially. Sweeping away from the duodenum can lead to serosal tears. The lateral attachments of the right colon are laparoscopically mobilized, being careful to stay in the lateral avascular plane.
ileocolic artery is grasped and elevated, and the avascular plane on either side is dissected free to allow clear visualization of the duodenum. The vessels are then ligated and divided using a vessel-sealing device such as the Ethicon EnSeal® (Ethicon Endosurgery, Cincinnati, OH) although the choice of the alternate energy source is up to the surgeons’ discretion. Care is taken at this point to sweep the duodenum medially. Sweeping away from the duodenum can lead to serosal tears. The lateral attachments of the right colon are laparoscopically mobilized, being careful to stay in the lateral avascular plane.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


