Fig. 41.1
The port that was added to obtain higher multiusability
41.2.2 Addition of Ports for Improving Manipulability and the Rationale of RPLS that Opposes Such Additions
The concept of RPLS conflicts with the history described above. RPLS represents an attempt to minimize the invasiveness of laparoscopic surgery by reducing the conventional number of four ports, including the additional port placed to achieve better manipulability. There is a concern that the manipulability may be increasingly sacrificed as the number of ports is reduced from four to three, and eventually to one. Some may consider this concept as representing “backward evolution.” In RPLS, which aims to reduce the number of surgical wounds, several trocars are inserted from the same incision to minimize the reduction in manipulability without affecting the number of manipulating forceps and scopes that can be used. Thus, this technique has many limitations that differ from those of conventional laparoscopic surgery. For example, the mobility of each device is impaired by the close proximity of the ends of the forceps and scopes, the trocar housing (head of the extracorporeal part), and the insertion of the devices from a single incision. Furthermore, the field of view is small because of the limited mobility of the scopes. Thus, it is undeniable that RPLS requires special techniques and skills that are substantially different from those of conventional laparoscopic surgery. Safety and reliability are critical, and only surgeons with a full understanding of these points should apply RPLS.
41.3 Current Status of RPLS in the Field of Gynecologic Surgery
SPLS was introduced in our department in March 2009. At first, it was applied to salpingectomy and salpingo-oophorectomy, which are based on the direct puncture technique and appear relatively easy in terms of the skill level required. When expansion of the indications was considered later, 2-port laparoscopic surgery was set as if the space between conventional 4-port laparoscopic surgery and SPLS was to be filled in consideration of the specific limitations of SPLS surgery described above [11].
In its early stages, SPLS was applied only to salpingo-oophorectomy and salpingectomy, which require fewer sutures. However, the indications have been expanded to include uterine myomectomy, total hysterectomy, promontory colposuspension, etc., by using the techniques described below. The following sections describe the actual surgical procedures.
41.3.1 Two-Port Laparoscopic Surgery
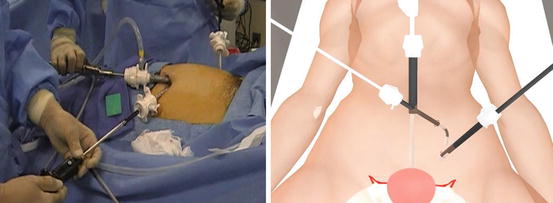
Figure 41.2 shows computer-graphics images of 2-port laparoscopic surgery. In 2-port laparoscopic surgery, the umbilicus is directly punctured with trocars for inserting the scope and manipulating forceps, and a 5-mm trocar is inserted via an incision made in the left inguinal region. The 5-mm port in the inguinal region can also be used for an incision for the insertion of a drain. When difficulty is encountered, incisions for the insertion of trocars are made at the same locations as in conventional 4-port laparoscopic surgery, so that trocars can be added in up to four ports in the same manner as in the conventional technique. Thus, even though up-conversion from SPLS to 2-port laparoscopic surgery and then to conventional 4-port laparoscopic surgery may be implemented, the location of the surgical wounds will consequently be the same as that in conventional surgery. When considering the burden on the patients, their satisfaction level, or the collateral for safety in the case of difficult surgery, the above points seem useful [11].
In 2-port laparoscopic surgery, the addition of an incision for trocars for SPLS allows auxiliary forceps to be inserted from a site different from that for the manipulating forceps and scope, allowing for surgery to be performed almost as easily as conventional laparoscopic surgery. Suturing, which is slightly difficult in SPLS, is simple, and 2-port laparoscopic surgery can be applied to myomectomy. Moreover, in both SPLS and 2-port laparoscopic surgery, attempts are being made to secure a good view while avoiding interference among the forceps and scopes by using flexible scopes manufactured by Olympus (Tokyo, Japan).
41.3.1.1 Uterine Myomectomy (2-Port)
Uterine myomectomy using the above 2-port laparoscopic technique is described here. Although it is performed in the same manner as the conventional 4-port laparoscopic technique, the forceps to be used by an assistant are unavailable. Because the surgery is performed with only a pair of forceps used by the surgeon, a few special techniques described below may be employed.
Securing a Good View Using a Flexible Scope
As described above, a flexible scope is used to avoid interference among devices that are inserted through trocars placed through a single incision. This is the same in SPLS. In the 2-port laparoscopic technique, a 12-mm trocar is placed at the umbilicus using the closed technique, and the scope is inserted. Under observation, a 5-mm trocar is placed in the inguinal region, and the scope is then placed in the 5-mm trocar. Under observation via the umbilical port, another 5-mm trocar is placed to intersect with the 12-mm trocar. Pneumoperitoneum leakage can be prevented by shifting the puncture site of the peritoneum. A flexible scope is inserted through the 5-mm trocar at the umbilicus. The view is secured as shown in Fig. 41.2, and surgery is performed. The forceps inserted from the trocar placed in the left inguinal region allow 2-port laparoscopic surgery to be performed in almost the same manner as that in conventional surgery.
41.3.1.2 Learning Curve in Acquiring the 2-Port Laparoscopic Technique
When 2-port laparoscopic surgery was introduced, the time needed to acquire the 2-port laparoscopic technique was examined for a single surgeon. The operation time decreased to a plateau with experience gained in approximately 8 cases (Fig. 41.3). Thus, the 2-port laparoscopic technique is fairly easy to acquire [12].
Fig. 41.3
This graph shows that the required operating time had stabilized within approximately 8 cases [15]
However, this technique also has its drawbacks. Because the surgery is performed with devices inserted via trocars placed at the umbilicus, there is no difference between sides. Although the posterior wall of the uterus and the Pouch of Douglas can be approached, the approach is somewhat difficult due to the distance between the entry site and the organs. Furthermore, because forceps inserted from the umbilicus make vertical contact with the posterior wall of the uterus during surgery, suturing is difficult. Thus, surgeons must be careful when performing either 2-port laparoscopic surgery or SPLS, which is described below, for a fibroid on the posterior uterine wall.
41.3.2 Single-Port Laparoscopic Surgery (SPLS)
While RPLS includes procedures using the direct puncture technique or various retractors, this section discusses SPLS. In the same manner as 2-port laparoscopic surgery, a flexible scope is used to secure the view. Furthermore, curved forceps, such as SILS™ (single incision laparoscopic surgery) forceps (Covidien, New Haven, CT, USA), are used to avoid interference among different forceps.
In the early stages of the introduction of SPLS we used the Roticulator graspers™ (Covidien). The release of dedicated SILS™ forceps (Covidien) has allowed SILS™ to be performed with superior manipulability. Furthermore, bendable automatic suturing devices, such as the SILS™ Stitch (Covidien), have also been made available. However, the use of disposable devices is disadvantageous in terms of the cost, and the SILS™ forceps (Covidien) are low in rigidity because they can be bent in the peritoneal cavity. As a solution, reusable, rigid, curved forceps, such as DAPRI forceps (Karl Storz–Endoskope, Tuttlingen, Germany) [13, 14] and YAMAGATA forceps (Adachi, Tokyo, Japan), have been introduced in the market. We have also developed and been using rigid forceps for gynecological use.
41.3.2.1 SPLS for the Uterine Adnexae
Salpingo-oophorectomy with the SLS technique is described here. Basically, ablation of ligaments with a sealing device facilitates the procedure. In this case, rigid forceps manufactured by Adachi industry were used (Fig. 41.4). Even for large cysts, the procedure can be applied after aspirating the contents of the cysts with a SAND balloon catheter (Hakko Co., Nagano, Japan). Because the incision in SPLS is of a certain size, it is easy to extract cysts from the body cavity.
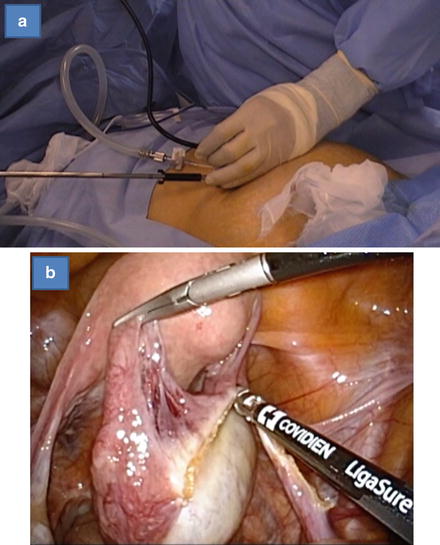
Fig. 41.4
(a) Direct insertion of reusable curved forceps ((Adachi) Industry Co. Ltd.) via SILS™ port (Covidien). (b) Salpingo-oophorectomy using vessel-sealing device and reusable curved forceps
41.3.2.2 Linear Salpingostomy with the SILS™ Stitch (Covidien)
Linear salpingostomy with the SILS™ Stitch (Covidien) refers to the surgery performed to resect pregnancy tumors and simultaneously to preserve the tubal patency in case of ectopic pregnancy [15]. Although extremely fine sutures are needed, the fascia and serosa are separately sutured using the SILS™ Stitch (Covidien) (Fig. 41.5).
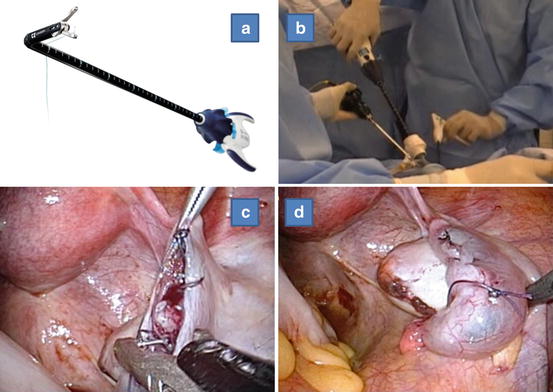
Fig. 41.5




(a, b) Use scenery of the SILS™ stitch (Covidien). (c, d) Linear salpingostomy using SILS™ stitch (Covidien)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
