Figs. 35.1 and 35.2
Preoperative axial CT image of the proximal porta hepatis
Figs. 35.3 and 35.4
Preoperative coronal CT image of the proximal porta hepatis
35.3.1 Resection of the Liver
35.3.1.1 Body Position and Choice of Incision
The patient should be placed in the supine position, and the great saphenous veins should be disinfected for stripping, when necessary. The Mercedes incision was chosen for abdominal exploration which range from right linea axillaris media and lateral margin of left rectus abdominis exoloma.
35.3.1.2 Abdominal Exploration
The various organs of the pelvic and abdominal cavities should be explored in the appropriate order to characterize the extrahepatic and perihepatic extent of disease.
35.3.1.3 Anatomy of the First Porta
Efforts should be made to avoid damaging the bile ducts, hepatic arteries, and portal veins, since the resected liver will ultimately be transplanted back in situ with anastomosis of the first porta (Fig. 35.5).
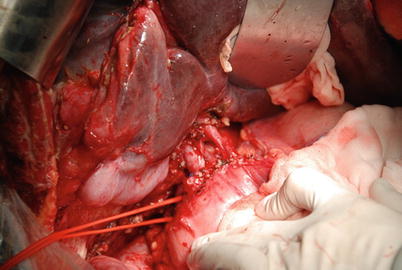
Fig. 35.5
Invasion of the first hilar structure
35.3.1.4 Lysis of the Perihepatic Ligaments
The perihepatic ligaments are usually invaded, especially the diaphragmatic muscle. Sometimes, part of the diaphragmatic muscle should also be resected (Figs. 35.6 and 35.7).
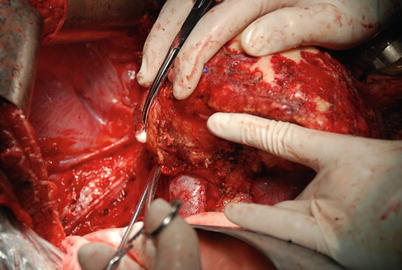
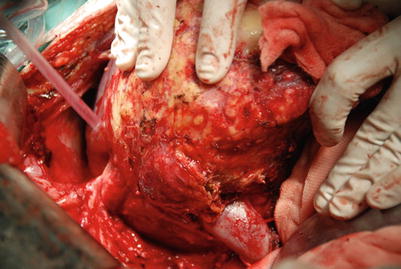
Fig. 35.6
Invasion of the diaphragmatic muscle and mobilization of the liver
Fig. 35.7
Invasion of the posthepatic inferior vena cava
35.3.1.5 Resection of the Liver
After mobilizing the perihepatic structures, resection begins. The structures should be transected in the following order: the bile duct, hepatic arteries, and portal veins in the first porta, then the posthepatic inferior vena cava, and finally, the suprahepatic vena cava and the liver.
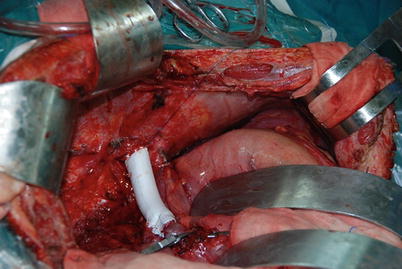
35.3.2 Reconstruction with an Artificial Blood Vessel
The resected part of the IVC was reconstructed with an artificial blood vessel. Then, an end-to-side anastomosis was created between the portal vein and the artificial blood vessel for the portacaval shunt. This can restore circulation in the portal venous system and stabilize the underlying circulation and the internal environment (Fig. 35.8).