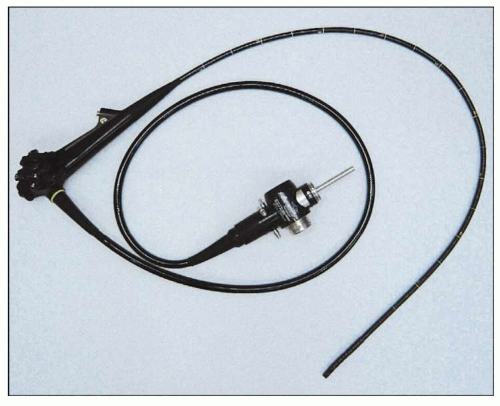
 2.1 The typical forward-viewing endoscope used for examination of the upper GI tract in an adult. Standard endoscopes range from 8-11 mm in diameter, and are from 100-160 cm in length. Controls allow for manipulation of viewing direction, air insufflation, suction, water spray, and taking still photos or video. |
 2.2 Side view close up. The two control knobs allow for four-way tip deflection. The outer/smaller dial is for right/left movement and the inner/larger dial for up/down movement. The biopsy channel allows for insertion of multiple instruments including biopsy forceps, brushes, electrocautery probes, snares, and sclerotherapy needles. |
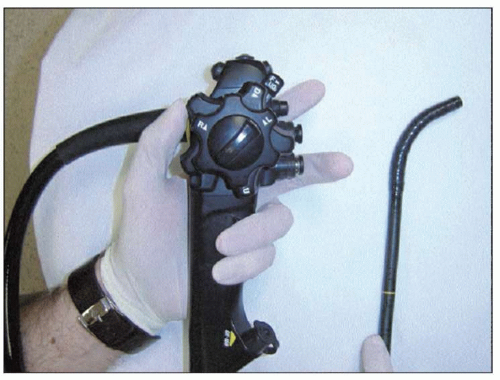 2.3 Rotating the inner dial up with the thumb causes the tip of the endoscope to deflect downward. |
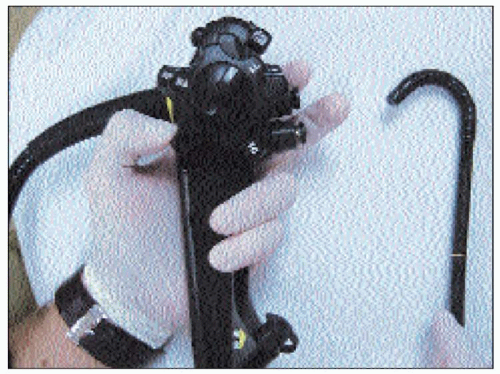 2.4 Rotating the inner dial down in the opposite direction causes the tip to deflect upward. Note the degree of deflection is not as great as when deflected downward. |
 2.5 Front view of the endoscopic controls. The two buttons allow for suction, water spray, and air insufflation. The forefinger is used to press the top button for suction. The second finger is usually employed to cover the second button resulting in air insufflation. Pressing this button will result in water spray. |
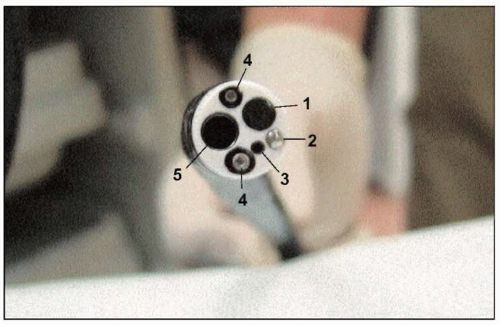 2.6 End view of the endoscope. Note the three channels for suction, insufflation, and instruments. Two light sources are also present. (1: video camera lens; 2: water flush nozzle for lens cleaning; 3: auxillary water channel; 4: light; 5: instrument channel.) |
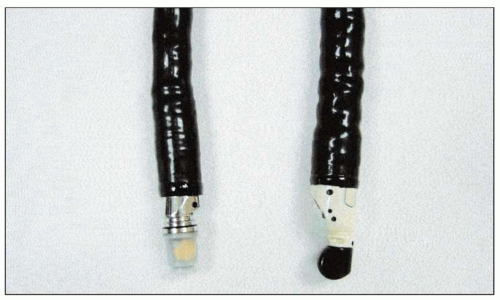
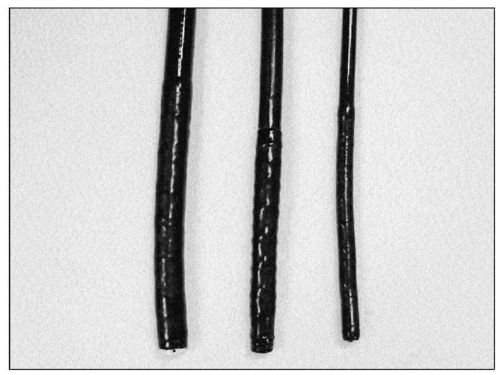 2.7 Upper GI endoscopes come in a variety of sizes. The small caliber endoscope (right), or ‘pediatric’ endoscope, has a diameter of 5-6 mm. It is ideal for use in children, but is also useful in adults with strictures or narrowings that the standard caliber endoscope cannot pass. These smaller instruments do have disadvantages, including decreased durability, poorer image quality, and smaller biopsy sizes. The larger ‘therapeutic’ scope (left) allows the passage of larger tools and more effective suction. |
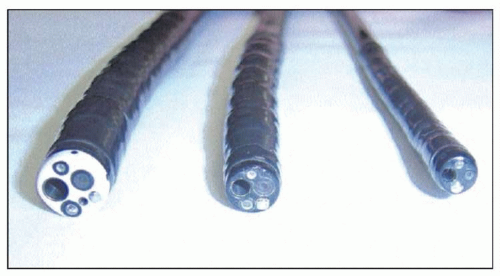 2.8 End view of instrument channel of different size endoscopes. Note the decrease in size of the channel from the therapeutic endoscope (left) to the small caliber endoscope (right). |
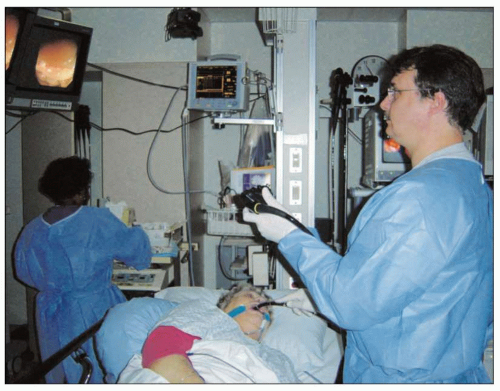 2.9 The patient is placed in left lateral decubitus position for proper positioning. The endoscopist stands directly in front of the patient’s mouth with the view screens located directly opposite. (Courtesy of John J Vargo, MD, Cleveland Clinic, Ohio, USA.) |
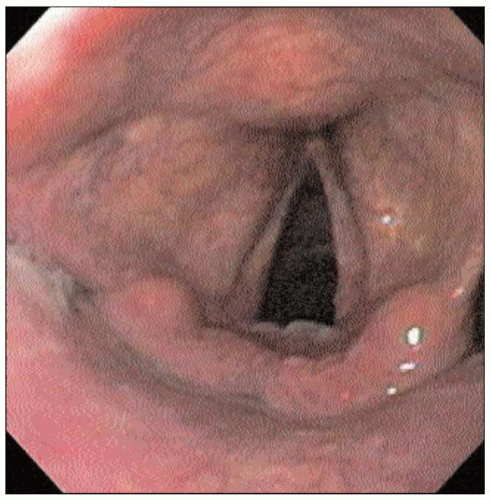 2.10 An endoscopic view of normal appearing vocal cords. This landmark is identified as an endoscopic exam begins, after the endoscope is passed through the incisors and over the tongue. Patients with extraesophageal reflux disease can present with symptoms, such as hoarseness, which can be caused by exposure of the vocal cords to gastric acid. Findings suggestive of reflux disease may include erythema, edema, granulomas, ulcerations, and laryngeal carcinoma. |
 2.11 Endoscopic appearance of the mid-esophagus during a normal examination. The squamous mucosa is pale and pink, without ulceration or inflammation. The lumen is of uniform caliber, and expands uniformly with air insufflation. Landmarks seen as the esophagus is traversed include pulsation of left atrium and aorta along with indentation from left mainstem bronchus. |
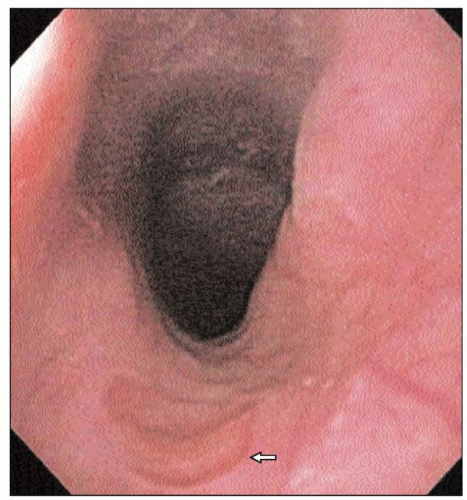 2.12 An esophageal inlet patch (arrow) is an area of heterotropic gastric epithelium found in the cervical esophagus. Note the darker red gastric mucosa, in contrast to the pale, pink esophageal mucosa. This is a common finding on upper endoscopy, and does not cause any symptoms in the patient. Inlet patches do not undergo malignant transformation, and usually no further follow-up is warranted. |
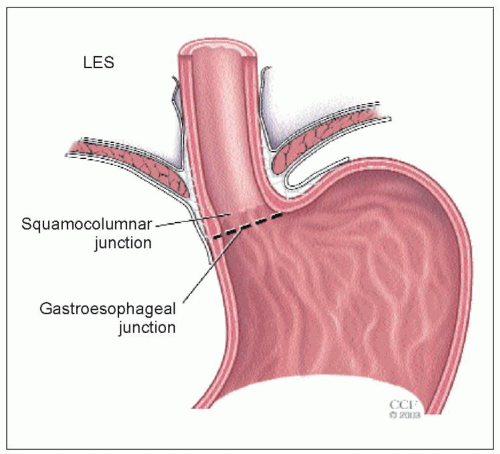 |
 2.14 An endoscopic view of a normal SCJ. The more proximal pale pink esophageal squamous mucosa meets the darker red gastric mucosa. The junction is irregular, and is called the ‘Z-line’. The location of the transition point more than 2 cm above the diaphragm signifies hiatal hernia. This junction is usually found at 38-40 cm from the incisor teeth in adults. |
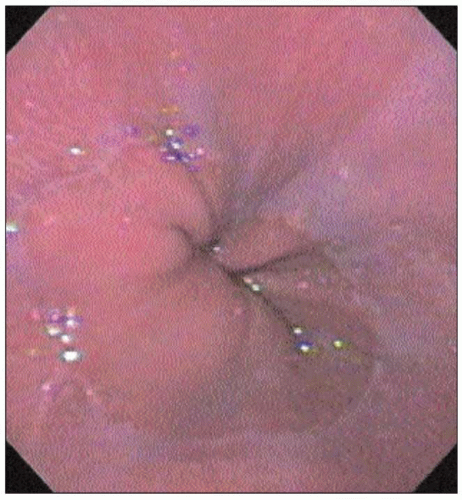
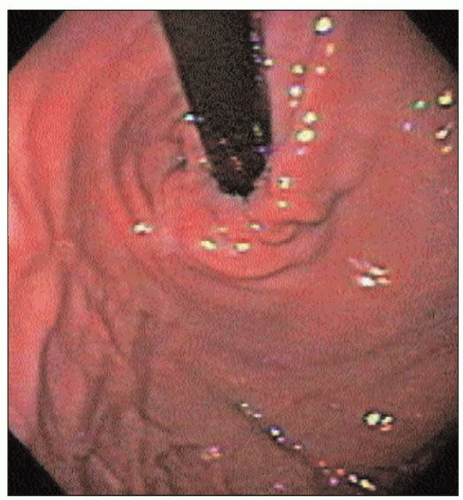 2.15 Gastric cardia on endoscopic retroflexion. Abnormalities to be noted include hiatal hernia, ulcers, gastric varices, and Mallory-Weiss tears. |
 2.16 View of echoendoscopes. The radial echoendoscope (left) has a rotating mechanical ultrasound probe that scans in a circle 90 degrees to the long axis of the scope. The linear echoendoscope (right) scans in the long axis of the scope. |
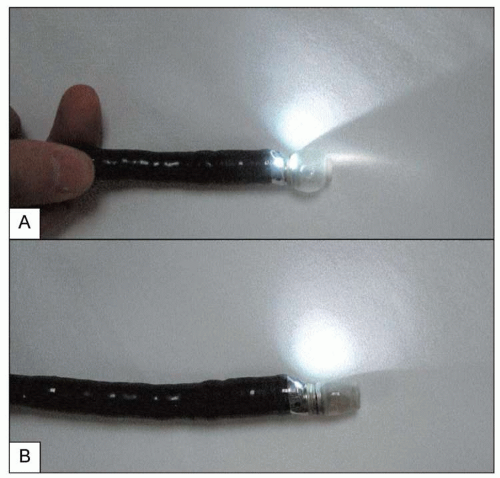 2.17 Balloon insufflation. A small latex balloon is placed over the ultrasound transmitter. With the balloon filled with water (A), better acoustic coupling can be achieved between the probe and the esophageal wall. This results in an improved ultrasound image. Note the light source is on which will provide an oblique endoscopic view. |
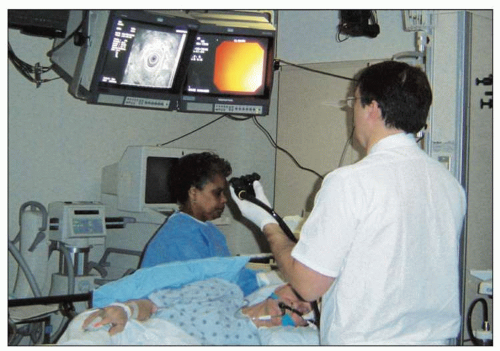 2.18 Two video screens are utilized: one screen shows the standard endoscopic image and the other the ultrasound image. (Courtesy of John J Vargo, MD, Cleveland Clinic, Ohio, USA.) |
Table 2.1 Endosonographic appearance of esophageal wall layers | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
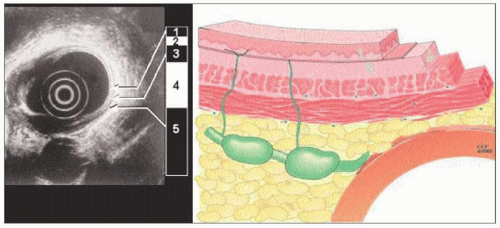 2.19 Schematic view of the esophageal wall and associated endoscopic ultrasound view. The endosonographic layers of the esophagus can be delineated as five alternating hyperechoic and hypoechoic bands that correspond to the histologic layers. The innermost layer is hyperechoic and corresponds to the interface between the ultrasound waves and the superficial mucosa. The second layer is hypoechoic and corresponds to the deep mucosa. The third layer is hyperechoic and corresponds to the submucosa. The fourth layer represents muscularis propria and is depicted as a hypoechoic band. The fifth layer is hyperechoic and represents the adventitia in the esophagus. |
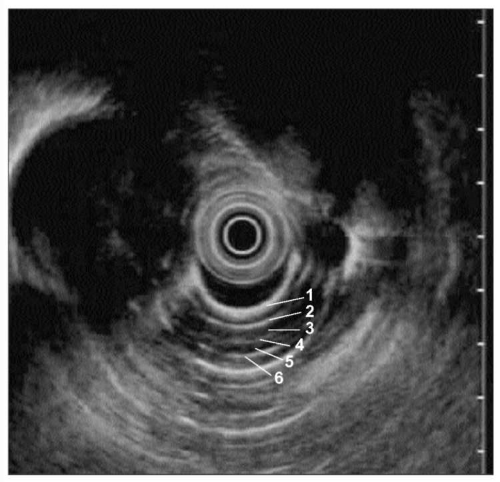 2.20 Normal endoscopic ultrasound, radial. (1: mucosa and muscularis mucosa; 2: submucosa; 3: inner circular smooth muscle; 4: intermuscular connective tissue; 5: outer longitudinal muscle; 6: adventitia.) |
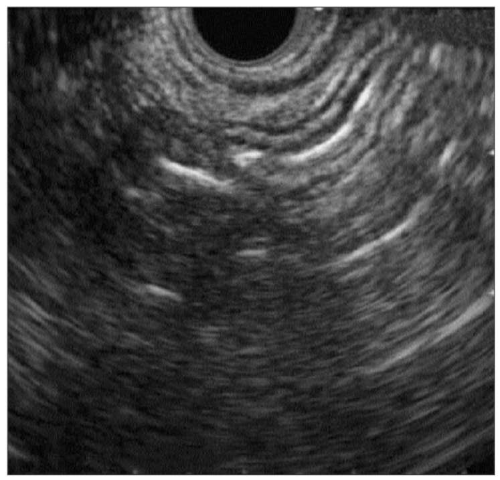 2.21 Normal endoscopic ultrasound, linear. (Courtesy of John J Vargo, MD, Cleveland Clinic, Ohio, USA.) |
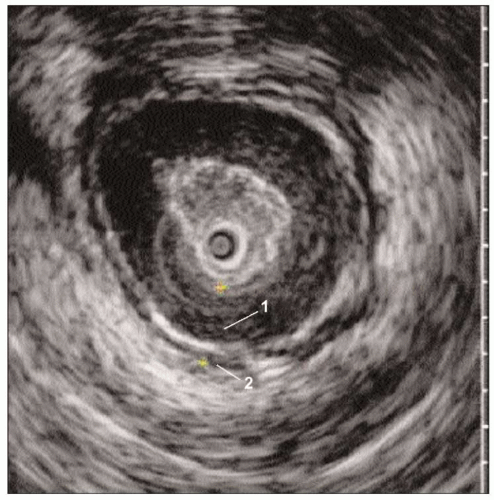 2.22 Endoscopic ultrasound of the LES. An echoendoprobe with higher frequency (higher detail, less penetration) can allow detailed visualization of the musculature of the LES. Note the hypoechoic inner circular and outer longitudinal layers separated by a thin band of hyperechoic material (1: inner circular smooth muscle; 2: outer longitudinal smooth muscle). |
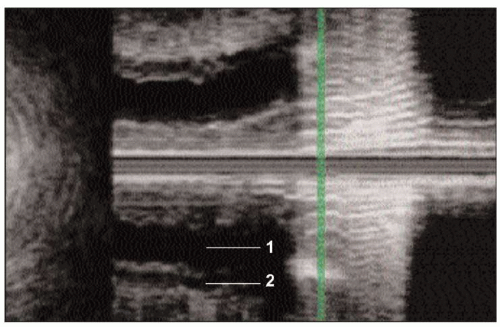 2.23 3-D Endoscopic ultrasound of the LES. Here the ultrasound image is reconstructed to a longitudinal view. Again note the two layers of the muscularis propria (1: inner circular smooth muscle; 2: outer longitudinal smooth muscle). |
Double contrast.
Full-column.
Mucosal relief.
Fluoroscopic observation.
Dysphagia.
Odynophagia.
GERD.
Esophageal strictures.
Esophageal motility disorders.
Esophageal function testing.
 2.24 Double contrast barium swallow. Double contrast barium swallow is performed by coating the esophagus with a dense barium and distending it with gas. This allows simultaneous examination of the distended esophagus and its mucosal surface. |
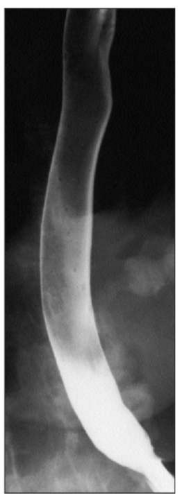
 2.25 Full-column barium swallow, obtained by rapid filling of the esophagus with barium while the patient is in the prone position. Esophageal motility may be assessed with fluoroscopy in the prone position by observing multiple swallows of barium. It is a good test to visualize hiatal hernias, lower esophageal mucosal rings, and peptic strictures. However, it may not detect small neoplasms, mild esophagitis, and esophageal varices. |
Evaluation of dysphagia in patients without evidence of mechanical obstruction, such as strictures, or in whom achalasia is suspected.
Defining the location of the LES for placement of intraluminal devices, such as a pH probe, which requires positioning relative to LES.
Pre-operative evaluation for anti-reflux surgery in patients suspected of having esophageal motility disorder such as achalasia.
Other possible indications are:
Table 2.2 Indications for esophageal manometry | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


