Chapter 58A Epidemiology of pancreatic cancer
Overview
Pancreatic ductal adenocarcinoma (PDA) accounts for 6% of all cancers in the United States. It is the fourth leading cause of cancer death in men, after lung, prostate, and colorectal cancer, and the fifth leading cause of cancer death in women, following lung, breast, colorectal, and ovarian cancer (Jemal et al, 2009). More than 42,000 incident cases of pancreas cancer are predicted annually, with about 35,240 deaths. Although mortality rates from pancreas cancer have improved slightly in the last decade, the diagnosis of PDA still confers an unfavorable prognosis.
Traditionally, PDA has been considered a predominantly male cancer; however, in 2009 the number of incident cases in women (21,420) exceeded the number of new cases in men (21,050) (Jemal et al, 2009). This suggests that the health consequences of increased smoking behavior by women over the last 3 decades are now becoming apparent. Pancreas cancer deaths remain higher in men (18,030) than in women (17,210), perhaps because of the presence of increased comorbidities or delayed diagnosis in men or greater genetic susceptibility to cancer, which limits treatment responsiveness in men (Jemal et al, 2009).
In the United States, the peak incidence of pancreas cancer occurs in the seventh and eighth decades of life (Horner et al, 2009). The U.S. population risk for pancreas cancer is 13.1 per 100,000 for men and 10.4 per 100,000 for women. The main risk for PDA occurs with advancing age. Between 2002 and 2006, the median age at diagnosis for cancer of the pancreas was 72 years, and the median age at death was 73 years according to Surveillance Epidemiology and End Results (SEER) data (Horner et al, 2009; SEER, 2010). Fifty-six percent of new PDA cases occur between the ages 65 and 84 years. The incidence of PDA remains highest for black Americans, with rates of 15.4 per 100,000 in men and 12.4 per 100,000 in women. The lowest risk of PDA is among Asian/Pacific Islander men and women (8.1 and 7.0 per 100,000, respectively). PDA is also a common second malignancy in both men and women who have had a prior smoking-related malignancy, such as lung or head and neck cancers (Neugut et al, 1995). The annual incidence rate worldwide for all histologic types of pancreas cancer is approximately 9 new cases per 100,000 persons (0.009), ranking it eleventh among all cancers.
In 2000, 217,000 new cases of pancreas cancer were reported globally, with 213,000 resultant deaths (Hariharan et al, 2008). The highest incidence of PDA in the world has been reported among Maoris in New Zealand, native Hawaiians, and black American populations; India and Nigeria have the lowest reported incidence (Boyle et al, 1989; Mack et al, 1985). In Europe during the same period, there were 60,139 incident cases with 64,801 deaths (Parkin et al, 2001). In Japan, PDA is the fifth leading cause of cancer death. Between 1950 and 1995, the worldwide incidence rates of PDA increased ninefold in men (1.4 to 12.5 per 100,000) and women (0.8 to 6.8 per 100,000), but rates have leveled off since 1985 (Lin et al, 1998). China reported 1619 deaths from pancreas cancer between 1991 and 2000, with rates higher in men and in urban areas compared with rural communities (Wang et al, 2003). No cases of PDA are reported in many African nations, reflecting the absence of an organized cancer registry system and an increased focus on more predominant causes of death in these nations. Incidence rates vary between 6 and 12 per 100,000 for the five Scandinavian countries, with Iceland having the lowest rates (Engholm et al, 2009).
Race And Ethnicity
African Americans
Combining all types of cancer, African Americans have the highest death rate (Ward et al, 2004) at 1.4 times higher than that of white males and 1.2 times higher than that of white females. In a 2004 study, Chang and colleagues (2004) used the California Cancer Registry of the Cancer Surveillance Section of the California Department of Health Services to determine the incidence of PDA between 1988 and 1998. African Americans had a higher age-adjusted incidence rate (8.8 per 100,000) for PDA when compared with all other races and ethnicities combined. African Americans were more likely to be seen with advanced disease and were least likely to receive surgical treatment, regardless of stage of disease (82.9% had no surgery compared with 77% of Asians, 67.8% of Hispanics, and 62.5% of non-Hispanic whites). Interestingly, serum cotinine levels, the primary metabolite of nicotine, are consistently higher in African Americans than in whites and Mexican Americans, even after adjustment for the number of cigarettes smoked per day, the number of smokers in the home, the number of hours of environmental tobacco smoke (ETS) exposure at work, the number of rooms in the home, and the region of the country where the subject lived (Caraballo et al, 1998). This suggests that genetic differences in cigarette product metabolism may influence rates of PDA.
Asians
Asian patients with PDA tend to have less aggressive tumors than do non-Asians (either black or white patients) and higher survival rates when assessed on a stage-adjusted basis (Clegg et al, 2008). To determine whether Asians develop a histologically different type of PDA than Western populations, Longnecker and colleagues (2000) conducted a population-based study using three SEER geographic areas: Hawaii, San Francisco, and Seattle. They compared PDA cases in Japanese, Chinese, Filipino, Hawaiian, black, and white patients. The study revealed that Japanese patients had the highest fraction of localized tumors with the lowest grade, and that Chinese, Filipino, and Japanese women had longer survival times than did whites, although survival time was significantly different for Japanese women only. Race-related genetic and environmental exposure factors may be involved in these survival discrepancies.
Ashkenazi Jews
Pancreatic cancer occurs in excess in Jews, particularly Jews of Ashkenazi heritage (Lynch et al, 1996). The age-standardized rates for PDA in Jews in Israel significantly exceed the rates for Israeli non-Jews (7.2 per 100,000 for all Jewish men and 5.7 per 100,000 for Jewish women vs. 4.0 per 100,000 for non-Jewish men and 2.9 per 100,000 for non-Jewish women). Approximately 5% to 10% of this discrepancy is attributed to the BRCA2 mutation, which is associated with breast, gastric, ovarian, and bile duct cancers.
Risk Factors For Pancreatic Ductal Adenocarcinoma
Our understanding of the risk factors for PDA continues to evolve. PDA is characterized by multiple germline and somatic genetic mutations (Hruban et al, 1998). This topic is covered extensively in Chapter 8A. It is estimated that less than 3% of pancreatic cancers are truly hereditary and due to inherited germline mutations and their respective syndromes (Wang et al, 2009). Other reported risk factors for PDA include cigarette, cigar, and pipe smoking; ETS exposure, also known as second-hand smoke or passive smoke exposure; exposure to occupational and environmental carcinogens; African American race; Ashkenazi Jewish heritage; high-fat, high-cholesterol diet; obesity; alcohol abuse; chronic pancreatitis; and long-standing diabetes (Table 58A.1; Gold et al, 1998; Everhardt et al, 1995; Silverman et al, 1994; Wynder, 1975).
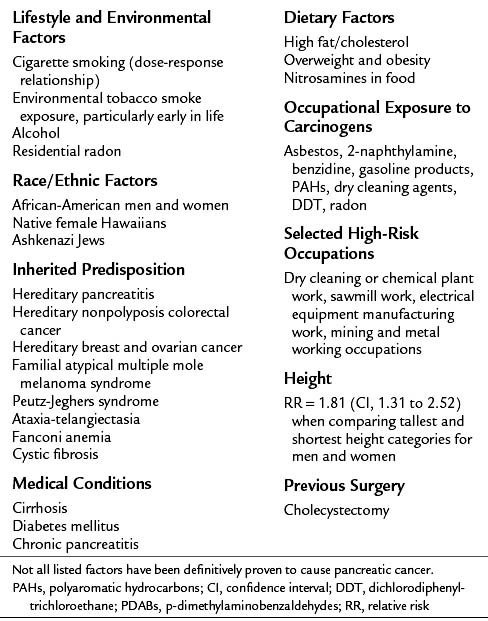
Data from Ahlgren, 1996; Efthimiou et al, 2001; Ekbom et al, 1994; Garabrant et al, 1993; Gold et al, 1998; Hruban et al, 1998; Kogevinas et al, 2000; Lowenfels et al, 1997; Lynch et al, 1996; Michaud et al, 2001; Silverman et al, 1998; and Yeo et al, 2009.
Familial Pancreatic Cancer
Family history of pancreatic cancer is a strong risk factor in 5% to 10% of cases (Lowenfels et al, 2005). When a history of PDA exists in a close relative, a number of responsible genes have been identified (Wang et al, 2009). In the National Familial Pancreas Tumor Registry (NFPTR) at Johns Hopkins, prospective studies of family members of pancreas cancer kindreds found a twofold increased risk of pancreas cancer in the first-degree relatives of persons with sporadic pancreas cancer and a ninefold increased risk in first-degree relatives of those with familial pancreatic cancer (Klein et al, 2004; Wang et al, 2009). Germline mutations of BRCA2 are found in 6% to 19% of familial pancreatic cancer patients (Murphy et al, 2002). When a more stringent definition of familial pancreas cancer is used, a 57-fold increased risk of PDA was reported in kindreds with three or more family members affected with PDA (Tersmette et al, 2001). This corresponds to an incidence rate of 301 cases per 100,000 per year compared with the SEER age-adjusted rate for the entire U.S. population of 8.8 cases per 100,000 per year. A recent report identified a germline truncating mutation of the PALB2 gene in 3% of familial pancreas cancer patients (Jones et al, 2009; Blackford et al, 2009). Despite these many advances in the understanding of the mutations involved in the pathogenesis of PDA, no single “pancreas cancer gene” has been identified.
Six Genetic Syndromes Associated with Pancreatic Ductal Adenocarcinoma
Six genetic familial syndromes and their respective predisposing genes have been identified and linked to the development of PDA; these are described briefly below (see also Table 58A.2). Although individuals with these syndromes have an increased risk of developing PDA, collectively these syndromes account for less than 5% of the familial aggregation of PDA. The mean age of onset of familial PDA is similar to that of nonfamilial cases: 65.8 years versus 65.2 years (Hruban et al, 1998). Familial cases have also been noted to have a somewhat increased incidence of secondary primary cancers (23.8%) when compared with their nonfamilial counterparts (18.9%).
Table 58A.2 High-Risk Genetic Disorders Associated with Familial Pancreatic Cancer
| Genetic Syndrome | Gene/Chromosomal Mutation Region | Estimated Increased Risk of PDA |
|---|---|---|
| Hereditary pancreatitis | PRSS1 (7q35) | 50 to 80 times |
| Hereditary nonpolyposis colorectal cancer (Lynch II variant) | hMSH2, hMSH1, hPMS2, hMSH3, hPMS1, hMSH6/GTBP | Undefined |
| Hereditary breast and ovarian cancer | BRCA2 (13q12-q13) | 3.5 to 10 times |
| FAMMM syndrome | p16 (9p21) | 20 to 34 times |
| Peutz-Jeghers syndrome | STK11/LKB1 (19p13) | 75 to 132 times |
| Ataxia-telangiectasia | ATM (11q22-23) | Rare |
FAMMM, Familial atypical multiple mole melanoma; PDA, pancreatic ductal carcinoma
Hereditary Pancreatitis
Children and adolescents with hereditary pancreatitis (HP) may develop severe pancreatitis at a young age, often in childhood or adolescence, with a resultant 50-fold to 80-fold increased risk of PDA developing over their lifetime. HP results from germline or new somatic mutations in the PRSS1 cationic trypsinogen gene (Lowenfels et al, 1997). Approximately 40% of those with HP will develop PDA when the additional risk factor of cigarette smoking is added. The risk of cancer seems to be limited to pancreatic cancers and not tumors in other organs.
Hereditary Nonpolyposis Colorectal Cancer
Hereditary nonpolyposis colorectal cancer (HNPCC) is an autosomal dominant inherited disease that predisposes affected persons to colorectal cancer and PDA (Hruban et al, 2002). It is usually caused by germline mutations in a number of DNA mismatch repair genes. Of the inherited syndromes associated with an increased risk of PDA, HNPCC is the least strongly linked to PDA.
Hereditary Breast and Ovarian Cancer
Patients with germline BRCA2 mutations have up to a 10-fold increased risk (range, 3.5 to ×10) of PDA developing even in patients without a strong family history of breast cancer. Goggins and colleagues (1996) identified germline BRCA2 mutations in 7% of sporadic (nonfamilial) PDA patients screened, none of whom had a family history of breast cancer or PDA.
Familial Atypical Multiple Mole and Melanoma Syndrome
Familial atypical multiple mole and melanoma (FAMMM) syndrome is rare condition associated with p16 germline mutations, a tumor suppressor gene that may be mutated or may have its expression altered by posttranscriptional methylation. The syndrome predisposes affected individuals to melanomas, multiple nevi, atypical nevi, and PDA (Lynch et al, 1990). Those with FAMMM have a 20- to 34-fold increased risk of PDA over their lifetime.
Peutz-Jeghers Syndrome
Peutz-Jeghers syndrome is a rare autosomal dominant disease associated with alterations in the STK11 gene, in which affected individuals develop hamartomatous polyps of the gastrointestinal tract and lip freckles referred to as mucocutaneous melanocytic macules (Hruban et al, 2002). Individuals with this syndrome have a roughly 100-fold increased risk of developing PDA (Giardiello et al, 2000), and they also appear to have a tendency to form intraductal papillary mucinous neoplasms (IPMNs).
Ataxia-Telangiectasia
Ataxia-telangiectasia is an autosomal recessive inherited disorder associated with ATM gene mutations, in which affected persons present with cerebellar ataxia, conjunctival telangiectasias, a hypofunctioning thymus gland, and oculomotor abnormalities. An association between ataxia-telangectasia and the subsequent development of PDA has been reported, but it is less well established than with the other five familial syndromes (Lynch et al, 1996).
Tobacco Exposure
Cigarette smoking is a contributing factor in approximately 20% to 25% of the cases of PDA and is the most consistently reported risk factor (Iodice et al, 2008; Jemal et al, 2009). Smoking has been associated with increased risk of PDA in at least 29 epidemiologic studies (Silverman et al, 1994), and smokers have a 70% increased risk of PDA compared with nonsmokers. Smoking habits in the 15 years preceding the diagnosis of PDA appear to be more relevant to increased risk, whereas former smokers who have quit for more than 13 years decrease their PDA risk to that of a lifetime nonsmoker (Howe et al, 1991).
Prospective and retrospective studies have found that the risk of PDA increases consistently with cigarette smoking but only inconsistently with cigar or pipe smoking (Wynder, 1975), suggesting perhaps that smoke must be deeply inhaled to exert its carcinogenic effects. A dose-response relationship between PDA and the number of cigarettes consumed has been documented in several investigations (Ahlgren, 1996; Howe et al, 1991). For current smokers who also have a family history of PDA, the relative risk of PDA has been reported to be as high as 8.23 (Schenk, 2001). Lowenfels and colleagues (1997) found that individuals with familial PDA tend to smoke more than those with sporadic PDA. These observations raise the possibility that smoking is interactive, perhaps multiplicatively, with genetic mutations known to be present in persons with familial PDA. Postmortem examinations of the pancreatic ducts of smokers have found widespread ductal hyperplasia, now called pancreatic intraepithelial neoplasia (PanIN), considered to be a premalignant lesion. Neugut and associates (1995) found a relationship between cigarette smoking and the development of PDA as a second malignancy in patients with a smoking-related first malignancy, such as lung, head and neck, or bladder cancer. This relationship is likely due to overlapping smoking-related genetic mutations among these different malignancies.
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
Preoperative and postoperative nutrition in hepatobiliary surgery
Medical management of bleeding varices: Primary and secondary prophylaxis
 Nonhepatic surgery in the cirrhotic patient
Nonhepatic surgery in the cirrhotic patient
 Liver transplantation for cholangiocarcinoma and other neoplastic diseases
Liver transplantation for cholangiocarcinoma and other neoplastic diseases
 Distal splenorenal shunt
Distal splenorenal shunt
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


