Fig. 10.1
The tip of the ESD knife is retracted within the sheath, and a mark is placed when the tip of the knife comes into contact with the mucosa
Mucosal Incision
The strategy for mucosal incision is dependent upon the endoknife type. When a Dual or Hook knife is used, basically the mucosal incision is performed from the oral side. At first, the backside of the hook knife is contacted with the mucosa, and a hole is made by Endocut I mode (Effect 3) (Fig. 10.2). After that, the tip of the hook knife is inserted into the submucosal layer, and the mucosa is hooked and cut with the hook part of the knife (Fig. 10.3). This is an important part of the process in order to prevent perforation. The arm part of the hook knife is used for longitudinal mucosal incision. The direction of the Hook knife is turned toward the esophageal lumen, and the knife is inserted into the submucosal layer by sliding the back side. Then the mucosa is captured by the arm part of the knife (Fig. 10.4), and, finally, the mucosa is cut with a combination of Spray coagulation (Effect 2, 60 W) and Endocut mode (Effect 3, duration 2, and interval 2). It is important in order to prevent bleeding during mucosal incision. The submucosal vessels cannot always be observed by endoscopy. Sometimes they are cut unexpectedly, and bleeding occurs during mucosal incision. Initial spray coagulation can coagulate submucosal vessels, and so such unexpected bleeding can be prevented with initial spray coagulation.
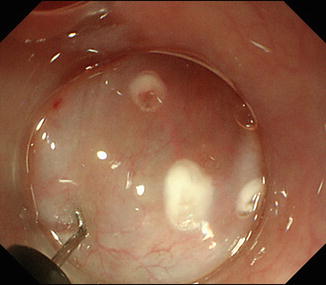
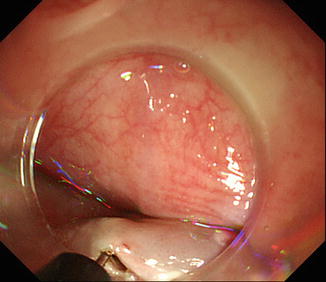
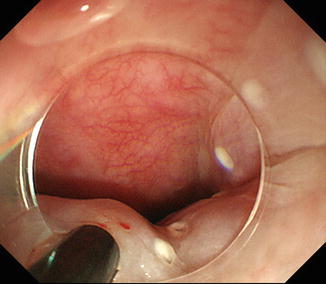
Fig. 10.2
The back side of the Hook Knife is placed so as to make contact with the mucosa, after submucosal injection of the fluid cushion, and a mucosal defect is made using the Endocut I mode
Fig. 10.3
The tip of the Hook Knife is inserted into the submucosal layer. The knife is used to hook and cut the mucosa
Fig. 10.4
The Hook Knife’s arm is used for vertical mucosal incision. The knife is directed toward the lumen and then inserted into the submucosal. The mucosa is then elevated toward the lumen with the knife’s arm, and then the mucosa is cut
A deeper cut of submucosal fibers is performed after mucosal incision. The Hook knife is inserted into the submucosal layer, and the submucosal fibers are hooked and cut. The lesion then shrinks by the contraction of muscularis mucosa (Fig. 10.5). After that, mucosal incision of the distal side is performed and then circumferential incision is completed. When an IT-nano knife is used, the mucosal incision should be started from the anal side. The initial mucosal incision at the anal side is made by a needle knife after submucosal injection. After that, the mucosal incision is made with IT-nano knife by Endocut mode. The operator cannot see the next mark well, because the cutting direction is always from distal to proximal. Therefore, the operator should take care to avoid cutting inside of the marks.
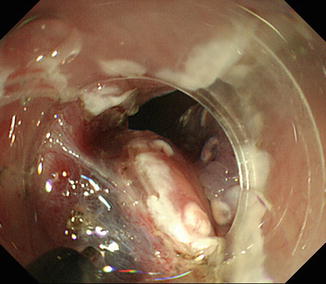
Fig. 10.5
The knife is inserted into the submucosal, and then the submucosal fibers are hooked and cut
Submucosal Dissection
The direction of gravity should be checked before submucosal dissection is started. Basically, submucosal dissection should be started from the lower side, because water and blood flow to the lower side causing the field of vision to become worse. Therefore, the operator should try to shift the lesion to the upper side. If submucosal dissection is begun from the upper side, the resected part will shift to the lower side, and submucosal dissection of the later half becomes difficult.
Tunneling Method
Tunnel-like dissection is necessary for circumferential ESD [12]. At first, a circumferential mucosal incision of the anal and oral parts is performed (Fig. 10.6). After that, a mucosal tunnel is made from oral to anal [12] (Figs. 10.7 and 10.8), and the second tunnel is made at the opposite side. Finally, the remaining submucosal fibers are dissected between the two tunnels (Fig. 10.9).
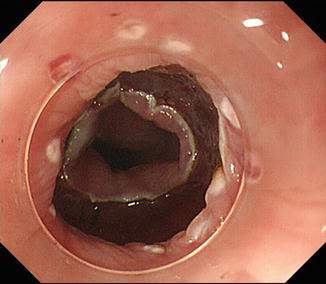
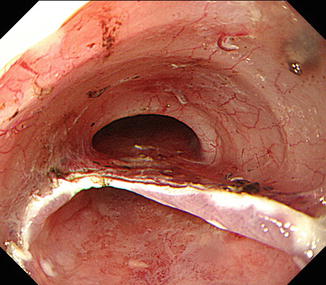
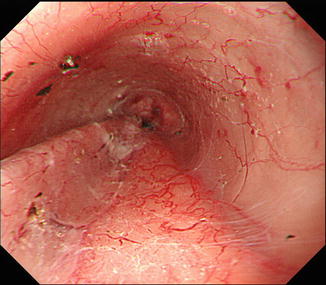
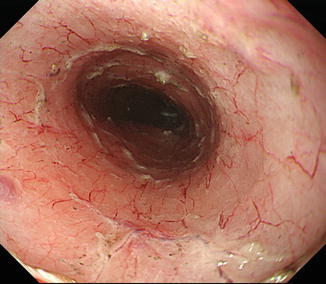
Fig. 10.6
Both oral and anal circumferential mucosal incisions were made
Fig. 10.7
After mucosal incision, a submucosal tunnel is made from the oral to anal side
Fig. 10.8
At the opposite side, a second submucosal tunnel is made. The submucosal fibers remaining between the two tunnels are subsequently dissected
Fig. 10.9
En bloc ESD upon completion
Clip-with-Line Method
If you can pull the target lesion, good countertraction can be made. The clip-with-line method was first reported in 2002 (Fig. 10.10) [13]. It is a simple and useful method for achieving countertraction during ESD. A long, 3-0, silk line is tied to the arm part of the clip (HX-610-135; Olympus, Tokyo, Japan) (Fig. 10.11). Then the clip-with-line is reset in the cassette. The scope is withdrawn when the circumferential incision is finished. A clip applicator device (HX-110QR; Olympus) is inserted into the accessory channel of the endoscope, and the clip-with-line is mounted onto the tip of the applicator. The scope is inserted again, and the submucosal side of the target lesion is grasped (Fig. 10.12). After that, the line is pulled very gently. Only a small amount of tension is required to create countertraction. This method also creates a clear field of vision (Figs. 10.13 and 10.14). During submucosal dissection, tension is maintained with a 10 g weight, such as a bite block mouthpiece, attached to the line. The 10 g weight creates sufficient countertraction and tension without threatening to tear the submucosal layer [14].

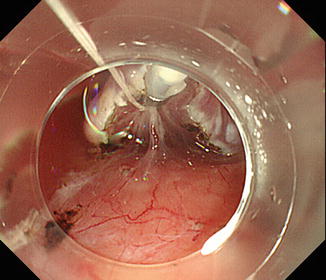
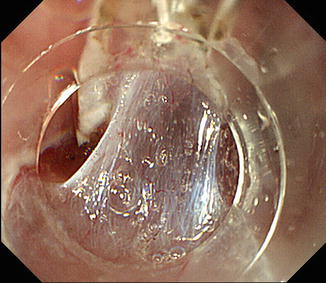
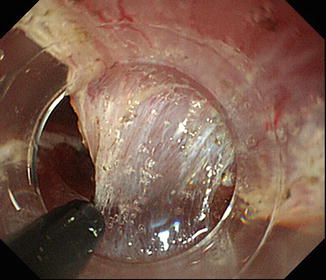
Fig. 10.10
Clip-with-line method. (a) A clip is placed at the distal edge of the target lesion once circumferential mucosal incision is complete. Countertraction and a clear field of view are obtained by pulling very gently on the line. (b) A second clip can be used to change the direction of the countertraction. (Originally from Oyama T, Yuichi K, Shimaya S, et al. Endoscopic mucosal resection using a hooking knife—intra gastric lesion lifting method. Stomach and Intestine. 2002;37:1159. Japanese with English summary)
Fig. 10.11
A long silk line is attached to the arm part of a clip (HX-610-135, Olympus, Tokyo, Japan)
Fig. 10.12
The clip is used to grasp the submucosal side of the target lesion
Fig. 10.13
Gentle pulling of the clip with traction line is used to provide countertraction
Fig. 10.14
Gentle pulling of the clip to provide countertraction facilitates submucosal dissection
Hemostasis
Bleeding makes the visual field worse; therefore hemostasis should be performed as early as possible. When bleeding occurs during mucosal incision or dissection, the area should be flushed to find the origin of bleeding.
Related posts:
 Management of Gastrointestinal EMR and ESD Perforation: From Lab to Practice
Management of Gastrointestinal EMR and ESD Perforation: From Lab to Practice
 Submucosal Fluid Cushion Injection Fluid: Western Perspective
Submucosal Fluid Cushion Injection Fluid: Western Perspective
 Submucosal Endoscopy: From ESD to POEM and POET
Submucosal Endoscopy: From ESD to POEM and POET
 Electrocautery for ESD
Electrocautery for ESD
 Advanced Endoscopic Imaging in the Upper Gastrointestinal Tract
Advanced Endoscopic Imaging in the Upper Gastrointestinal Tract
 Role of EUS on Preoperative Staging of Gastric Cancer for ESD
Role of EUS on Preoperative Staging of Gastric Cancer for ESD
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


