Appendicitis, Diverticulitis, and Colitis
Keywords
• Appendicitis • Diverticulitis • Colitis • Inflammatory bowel disease • Clostridium difficile • Emergency medicine
Appendicitis
Overview and Epidemiology
Appendicitis is the most common cause of abdominal pain requiring surgical intervention. The lifetime risk of appendicitis is approximately 7%, with a current incidence of 86 per 100,000 patients per year.1 Rates of appendicitis are highest in the second decade of life, with a slightly higher incidence of appendicitis occurring in males (ratio 1.4:1).2 Appendiceal perforation rates also vary; patients at extremes of age are more likely to have perforated at their time of diagnosis.1 Early diagnosis of appendicitis is paramount, because patient morbidity is increased once appendicitis becomes complicated by abscess and perforation.
Pathophysiology
The appendix is located on the posteromedial surface of the cecum, approximately 3 cm from the ileocecal valve. Its length varies from 8 to 13 cm, and its anatomic location within the abdomen is variable.3 Although the appendix has no known function, recent studies propose that it acts as a reservoir for commensal bacteria in the colon.4
Appendicitis occurs when the appendiceal lumen becomes obstructed by fecaliths, adhesions, enlarged lymph nodes, foreign bodies, parasites, or, less commonly, tumors.5,6 Once obstruction occurs, the intraluminal pressure within the appendix begins to increase as mucosal secretions accumulate, leading to appendiceal distension. This distension in turn stimulates visceral afferent nerves that enter the spinal cord at the T8 to T10 level, causing dull epigastric or periumbilical pain. As obstruction continues, pressures within the appendix impede venous and lymphatic drainage, allowing bacteria and neutrophils to invade the walls of the appendix. More localized pain occurs after continued inflammation within the appendiceal serosa causes irritation of local somatic fibers on the parietal peritoneum. If this process remains unchecked, the appendix becomes gangrenous and is at risk for perforation, abscess formation, and peritonitis, often within 24 to 36 hours of symptom onset.7
Clinical Presentation
Classically, a patient with appendicitis presents with constant pain that is poorly localized to the periumbilical or epigastric region, and is accompanied by anorexia, nausea, and vomiting. Vomiting usually begins after the abdominal pain. Illness progression leads to migration of pain to the right lower quadrant at the area of the McBurney point, and can be accompanied by low-grade fever. A meta-analysis evaluating patients with abdominal pain reported an increased likelihood of appendicitis when the patient’s pain was located in the right lower quadrant, had migrated from the periumbilical region, and had been accompanied by fever.8
However, this classic clinical presentation is not always present, partly because of the variability of the appendiceal location within the abdomen. For example, the appendix may lie in a retrocecal, retroiliac, or pelvic location, leading to pain in the right flank, pelvis, testicle, suprapubic region, or even left lower quadrant if the appendix crosses the midline. Likewise, patients may experience dysuria, urinary frequency, diarrhea, or tenesmus depending on the location of the inflamed appendix. These varied positions of the appendix and their associated complaints can delay the early diagnosis of appendicitis and increase the risk of gangrene and perforation.9
Multiple physical examination findings exist to aid in the diagnosis of appendicitis. Pain with palpation is classically found at the McBurney point, located “exactly between an inch and a half and two inches from the anterior spinous process of the ileum on a straight line drawn from that process to the umbilicus.”10 A positive Rovsing sign is present when palpation of the left lower quadrant elicits tenderness in the right lower quadrant. Patients may also show rebound tenderness or guarding, which are responses to the inflamed parietal peritoneum, and, when present, have been found to be independent predictors of appendicitis.11
Additional signs can aid in the physical diagnosis. The psoas sign is performed either by having the patient flex at the right hip against resistance, or by extending the hip with the patient in the left lateral decubitus position, thereby irritating the iliopsoas muscle. A positive obturator sign is present when internal rotation of the flexed right hip with the knee in flexion exacerbates the patient’s pain. A rectal examination is often performed, although the sensitivity and specificity of rectal tenderness for appendicitis are weak.8
Temperature is either normal or slightly increased early in the course of appendicitis. Patients may develop fever as the disease state progresses toward perforation and abscess formation. Therefore, temperature increase alone cannot rule in the diagnosis of appendicitis, but the presence of a fever, when taken in concert with other history and physical examination findings, such as migration of pain, can make the diagnosis more likely.8
Special populations
Pregnancy
In theory, the gravid uterus can displace the inflamed appendix cephalad and lead to right upper quadrant or right flank discomfort. However, most pregnant women with appendicitis present with right lower quadrant pain, regardless of their stage of pregnancy.12,13 There is a slightly higher incidence of appendicitis in the second trimester compared with the first and third.14 Although pregnant women are not at increased risk for appendicitis compared with nongravid controls, appendicitis is the most common nonobstetric surgical emergency in pregnancy. Early recognition in the pregnant patient with appendicitis is important because complications such as peritonitis or abscess formation can affect fetal outcomes. Studies have shown high rates of fetal loss in both uncomplicated and complicated appendicitis (15% and 37%, respectively). Pregnant women are also at risk of early delivery, with some series showing rates reaching 45%, although recent data show improvement in these outcomes.15,16
Children
Young children and the aged are also at risk for delayed diagnosis of appendicitis and its complications, and therefore a high index of suspicion is necessary when evaluating these populations. Studies have found pediatric patients to be initially misdiagnosed with gastroenteritis, urinary tract infection, otitis media, or respiratory infections, ultimately increasing perforation rates (approximately 70%–80%) and hospital lengths of stay.17–19
Elderly
Likewise, elderly patients tend to have a delay between symptom onset and treatment of appendicitis. This delay leads to increased rates of perforation. Mortality from appendicitis in the aged increases to 4% from 0.1% for younger patients, and is particularly high in those greater than 70 years of age (32%). Reasons for delay in diagnosing this population include misdiagnosis and atypical patient presentation,20,21 although more recent data show early computed tomography (CT) scanning and laparoscopy are improving outcomes.22
Immunocompromise
Immunocompromised patients, such as those with acquired immune deficiency syndrome (AIDS), are also at risk for complications from appendicitis, partly because of the similar symptoms that opportunistic infections can cause in this population. Although patients with AIDS have been found to present with typical symptoms of appendicitis, these symptoms may be misattributed to opportunistic infections or other AIDS complications. However, patients with AIDS are more likely than those without the disease to be perforated at the time of surgical intervention.23 Recent retrospective data suggest that antiretroviral therapy may play a protective role in the development of appendicitis in patients with AIDS.24
Diagnosis
Laboratory
The clinical usefulness of a white blood cell (WBC) count with differential remains uncertain. In one recent series, an increased WBC count of greater than 10,000 cells/mm3 had a sensitivity of 76% and specificity of 52%.25 This is similar to other data showing that leukocytosis alone is a poor predictor of appendicitis and does not distinguish between simple versus complicated cases.26 The inflammatory marker C-reactive protein (CRP) has been shown to have both a low sensitivity and low specificity when used alone in appendicitis evaluation.27,28 However, the combination of leukocytosis, leftward shift, and increased CRP may be more useful than each test alone in the diagnosis of appendicitis. A recent meta-analysis showed an increased likelihood of appendicitis when 2 or more of these studies were increased and a decreased likelihood when all 3 were within normal limits.29 Therefore, laboratory testing should be seen as an adjunct to other elements of the history and physical examination when appendicitis is suspected, but cannot definitively make the diagnosis.
Imaging
Multiple imaging studies in the evaluation of appendicitis exist, although the usefulness of each study can vary. Plain films are seldom used in the diagnosis of appendicitis; however, they can help rule out other causes of abdominal pain (volvulus, intussusception, or nephrolithiasis) and may be performed rapidly at the bedside. Signs suggestive of appendicitis on radiograph include localized paralytic ileus, gas or fecalith in the appendix, blurring in the area of the right psoas muscle, and free air, although no sign is sensitive or specific in making the diagnosis,30 which limits the value of plain film in this disease.
Ultrasound
Ultrasound can be a useful test in the evaluation of appendicitis, particularly in children and pregnant women in whom there are particular concerns regarding ionizing radiation. The sensitivity of graded compression ultrasonography is as high as 98% (although these numbers vary widely between studies)31 and is considered positive for appendicitis when the diameter of the appendix is greater than 6 to 7 mm (Fig. 1).27,32,33 Inflammation surrounding the appendix, appendicoliths, or hyperemia of the appendiceal wall can also be visualized by ultrasound in the setting of acute appendicitis. False negatives can occur once the appendix has perforated, thus reducing the diameter of the appendix, or when the appendix is retrocecal or inflammation is confined to the tip of the appendix.34 Another challenge in using ultrasound is that the appendix cannot always be visualized. Even using skilled sonographers, the appendix is not visualized between 25% and 35% of the time,27,33 which can be partly caused by patient’s body habitus or bowel gas overlying the appendix. The negative predictive value of a nonvisualized appendix on ultrasound is 90%.27 Thus, although a positive ultrasound is diagnostic of appendicitis, a negative ultrasound in which the appendix is not seen cannot rule out the diagnosis of acute appendicitis, and other diagnostic tools should be used.

Fig. 1 Ultrasound shows an enlarged appendix with a fluid-filled lumen.
(From Paterson A, Sweeney LE, Connoly B. Paediatric abdominal imaging. In: Grainger R, Allison D, eds. Grainger & Allison’s Diagnostic Radiology: A Textbook of Medical Imaging. 5th Edition. Philadelphia: Churchill Livingston, 2008; with permission.)
CT
CT has become widely used in the evaluation of suspected appendicitis. Advantages include its widespread availability as well as its capacity to detect other abdominal disorders. Disadvantages include patient radiation exposure, time delay to diagnosis if oral contrast is used, and risk of contrast-induced nephropathy or contrast reaction when intravenous contrast is used. Some investigators consider increased cost to be a disadvantage of this imaging modality, but data have suggested a decrease in the rates of unnecessary appendectomy since CT scan use has increased.35 Findings suggestive of acute appendicitis on CT scan include an enlarged appendix with diameter greater than 6 mm, appendiceal wall thickening, and pericecal inflammation (Fig. 2). An appendicolith alone is not sufficient to make a radiographic diagnosis of appendicitis.36

Some controversy exists about the use of contrast in the evaluation of appendicitis on CT. The sensitivity (83%–97%) and specificity (93%–98%) of CT in acute appendicitis vary with the presence or absence of contrast, as well as type of contrast used. A recent review article found the sensitivity and negative predictive value of CT without oral contrast to be equal to that of CT with oral contrast; the specificity, accuracy, and positive predictive value of CT without oral contrast was superior to that of CT with oral contrast in this analysis.37 The implication of this review may have important ramifications on emergency department (ED) length of stay and may decrease time until surgical intervention for patients. Other studies have shown the sensitivity of noncontrast scans to be greatly inferior to those using contrast.38
Another promising option uses rectal contrast only. In a series of 100 patients, CT with rectal contrast had a sensitivity, specificity, positive and negative predictive values, and accuracy of 98% in diagnosing acute appendicitis.39 More recent prospective data have shown more modest outcomes for this modality, but imply that rectal contrast studies can be useful in the evaluation of acute appendicitis.38 Perhaps the best approach to the use of contrast in patients suspected of having appendicitis should take into account the breadth of the differential diagnosis. Oral and intravenous contrast may help better delineate other causes of abdominal pain (particularly in young women) and should be considered when the diagnosis of appendicitis is uncertain. Establishing an institutional protocol with respect to contrast administration may also aid in the decision of whether contrast should be used, and by what route.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) may also have a limited role in the work-up of appendicitis. Unlike CT, MRI does not expose patients to ionizing radiation. It is therefore considered safe in pregnancy. Gadolinium crosses the placenta and should therefore be avoided, particularly in the first trimester. Disadvantages include limited availability, high cost, and lengthy scan times. If obtainable, MRI may be a good second-line imaging study when a pregnant patient has an indeterminate ultrasound.40
Clinical scoring
Several scoring systems have been developed in an attempt to assist in the diagnosis of acute appendicitis. The most often cited is the MANTRELS score, which is a mnemonic that uses 8 different variables on a total 10-point scale.41 These variables include migration of pain, anorexia, nausea or vomiting, tenderness in the right lower quadrant, rebound tenderness, elevation of temperature, leukocytosis, and leftward shift. The score may aid clinicians in deciding which patients can be observed and which require operative intervention. It has also been shown to be helpful in discriminating between patients who require imaging for suspected appendicitis and those who may be discharged without imaging.42
Treatment
A recent review article confirms that antibiotics can prevent postoperative wound infection in uncomplicated appendicitis and minimize abscess formation in cases of perforation.43 Antibiotic therapy should include coverage for enteric gram-negative organisms as well as anaerobes, and should be considered in conjunction with the consulting surgeon. Possible regimens include a second- generation or third-generation cephalosporin for uncomplicated cases. In the event of abscess formation or perforation, broader-spectrum coverage with a medication such as piperacillin-tazobactam or a 3-drug regimen including a cephalosporin and aminoglycoside along with metronidazole is warranted.44
A study investigating antibiotic and medical management versus appendectomy showed that, although most patients improved in the short term with medical management, greater than one-third of patients required surgery for recurrent appendicitis within a year.45 Therefore, operative intervention remains the definitive treatment of acute appendicitis, and early surgical consultation is necessary. In cases of abscess formation at time of presentation, surgeons may opt for initial percutaneous abscess drainage initially, followed by interval appendectomy.
Diverticulitis
Overview and Epidemiology
Diverticular disease is commonly seen in the adult population. The overall prevalence of diverticulosis has been reported to be roughly 27% and increases with advancing age.46 Of those patients with symptoms from diverticular disease, 3% are less than 40 years of age, whereas each decade between the ages of 50 and 70 years accounts for approximately 25% to 30% of cases.47 The prevalence is much higher in developed countries, and is believed to be partly the result of physical inactivity48 and a low-fiber diet.49 Symptomatic disease, including diverticular pain and diverticulitis, occurs in roughly 10% to 25% of patients with diverticulosis.50
Pathophysiology
Diverticula are small outpouchings or herniations that form at areas of weakness in the wall of the colon. In general, they are located at the vulnerable areas in which the vasa recta enters the muscularis. Except for diverticula of the cecum, which comprise all 3 layers of the colonic wall, most acquired diverticula contain mucosa and submucosa only. Diverticular disease affects the left-sided and sigmoid colon more than 90% of the time.51 Although many causes of diverticulosis have been proposed, the exact cause of the condition is not known. Problems of colonic motility and muscular abnormalities of the colon wall are possible causes. Another hypothesis is that diverticulosis is a disorder arising from increased intraluminal pressure.52 Although diverticulosis is largely an asymptomatic condition, these areas can perforate and become inflamed, leading to diverticulitis.
Patients can have either complicated or uncomplicated episodes of diverticulitis, which has ramifications for treatment as well as patient morbidity. Complicated cases are those in which there is perforation, obstruction, abscess, or fistula formation.53
Clinical Presentation
Patients with acute diverticulitis may also present with right-sided abdominal symptoms. This possibility applies particularly to Asian54 and younger55 patients, who are more likely to have proximal colonic disease. In addition, redundant sigmoid colon may be present on the right side of the abdomen, leading to right-sided symptoms in patients with distal colonic disease.
A high index of suspicion is necessary when evaluating patients who are elderly or immunocompromised. These groups may present with less-impressive symptoms and physical examination findings. As a result, they are more likely to have perforation at the time of diagnosis.56,57
Diagnosis
Imaging options are available when the diagnosis of diverticulitis is uncertain, or if suspicion exists for complications of diverticular disease. Contrast enema has typically been considered the gold standard in diagnosis, although it is falling out of favor as a first-line study. Although contrast enema is able to diagnose diverticulitis, it is unable to assess for the presence of an abscess and cannot determine the severity of inflammation.58 Thickened colonic folds, contrast extravasation, and localized mass effect may be seen on contrast radiography.59 Fistula formation may also be evident. The use of non–water-soluble contrast material in colonic contrast studies can also lead to problems associated with intraperitoneal barium when perforation is present, and should therefore be avoided in patients with signs of local peritonitis on examination. If this type of imaging is used, it is best to use water-soluble contrast.
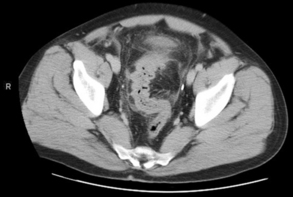
CT is the study most used for the diagnosis of diverticulitis. CT with both oral and intravenous contrast has the advantage of being able to evaluate the colonic walls as well as extraluminal areas, in addition to being able to assess for other causes of abdominal pain. The sensitivity of CT for diagnosis of diverticulitis ranges from 85% to 97%.60 Positive findings of diverticulitis include thickening of the bowel wall and fascia, pericolic fat stranding, and local abscess formation (Fig. 3).61






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


