Fig. 9.1
(a) 5-mm low profile trocars (Karl Storz-Endoscope). The use of low profile trocars enables improved avoidance of instrument collision and better maneuverability. (b) Three low profile trocars inserted through a single 18-mm skin incision during a SPLS cholecystectomy. Note staged insertion of the trocars into the abdominal wall to minimize their collision with one another
9.2.2 Improvised Access Device: The Glove Port
Several studies have reported an improvised technique to access the abdominal cavity through a single incision, with the application of a surgical glove. Hayashi et al. and Livraghi et al. reported on a series of SPLS (mainly cholecystectomies and appendectomies) using a standard wound protector covered with a surgical glove with several small incisions made on the tips of the glove-fingers to induce pneumoperitoneum and to create working channels for the laparoscopic instruments [16, 17]. The authors described this technique as having multiple advantages: easy to use, simply accommodated to the abdominal wall even in overweight patients, allows simultaneous passage of a maximum of 5-mm instruments and allows a wide axis of movements and hence minimizes instrument collision. The low cost of the application of this technique is mentioned as a potential advantage as well. Eumatsu et al. as well as Ishida et al. applied a similar technique for SPLS colectomies and concluded it is safe and feasible [18, 19].
Although the glove port technique may be safe and feasible, in the era of standartization and strict FDA control of medical devices, this technique may be used only in countries free from FDA/CE mark device approvals.
9.2.3 Dedicated Access Devices
A variety of dedicated access devices are available. These devices offer different solutions to the challenges mentioned above. Some are reusable, but most are disposable and thus increase the overall OR cost.
The SILS™ port (Covidien, New Haven, CT, USA) is a disposable access port. It has a firm foam-like consistancy and is inserted through a 2-cm fascial incision. The port adjusts to the wound edges and retracts the abdominal wall to provide an airtight seal. Through this port 5/12-mm trocars and instruments can be passed into the peritoneal cavity (Fig. 9.2).
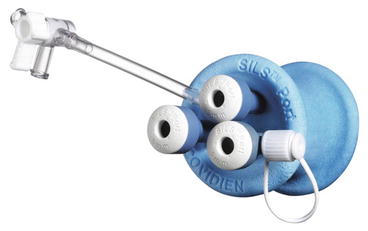
Fig. 9.2
SILS™ port (Covidien)
The GelPOINT® (Applied Medical, Rancho Santa Margarita, CA, USA) has a disposable gel platform connecting to an adjustable polyethilene sheath which has an inner and external rings (Fig. 9.3). This sheath serves also as a standard wound protector while extracting organs. The gel platform enables insertion of several dedicated or standard trocars wide apart from each other lowering the incidence of instrument collision.

Fig. 9.3
GelPOINT® access device (Applied Medical)
The Triport® and Quadport® (Advanced Surgical Concepts, Wicklow, Ireland) are disposable devices. Both have a similar adjustable plastic sleeve which is inserted through a 2-cm fascial incision using a special introducer. The sleeve is then connected to an external cap with different configurations of several valves allowing passage of rigid and curved instruments into the abdominal cavity (Fig. 9.4).

Fig. 9.4
Quadport® acces device (Advanced Surgical Concepts)
The X-Cone™ (Karl Storz-Endoscope, Tuttlingen, Germany) is a rigid reusable port, which consists of two metallic parts and a reusable silicone cap (Fig. 9.5). The port is assembled following the positioning of both metallic parts through the incision, thereby creating an air tight seal and maintaining constant fascial incision length. The silicone cap contains three flexible ports enabling the passage of rigid and curved instruments, and two more ports, which have no profile height to reduce the space occupied by the ports. In total the port offers introduction of five instruments. The special rigid hourglass configuration facilitates the use of curved instruments to achieve adequate retraction and triangulation.

Fig. 9.5
X-Cone™ (Karl Storz-Endoscope), a reusable SPLS access device
The Single Site Laparoscopy Access System (Ethicon Endosurgery Inc., Cincinnati, OH, USA) is a disposable port. It has a plastic sheath in various sizes that is inserted through the incision using a dedicated introducer. A unique rigid cap is then connected to the external ring of the sheath, which has three entry ports (Fig. 9.6). These ports are the seal mechanisms only without any tubing or trocars thereby maximizing the space offered for instruments and motion around the cap.

Fig. 9.6
Single site laparoscopy access system (Ethicon)
Several other devices are on the market like the ENDOCONE™ (Karl Storz-Endoscope), the S-Port® (Karl Storz-Endoscope), the X-Gate (Ethicon) and more. Most have similar designs with minor changes that differentiate them.
9.3 Cameras
As mentioned above, the view is compromised in SPLS, due to the common point of entry of instruments and camera into the abdominal cavity. The passage of instruments within the camera’s visual field obscures the surgical field and creates a challenge. Excellent coordination and communication between the surgeon and the camera operator is crucial to the success of SPLS, but sometimes it is not enough. The consortium for LESS surgery has stated in their consensus statement that “the surgeon should be able to visualize structures from differing perspectives, preferably offline from the axis of the instruments” [15]. In an attempt to overcome the challenge of a compromised view, different cameras and endoscopes were evaluated.
9.3.1 Rigid Laparoscope
The rigid laparoscope is the most commonly used endoscope for SPLS, as in any other laparoscopic surgery. The use of a 30 degree laparoscope is highly recommended if a rigid laparoscope is being used, this is due to its ability to deviate from the axis of the instruments while viewing the surgical field [14, 20].
Standard telescopes are 30 cm in length, and this might exacerbate the challenge of instruments’ “sword fighting”, especially outside the abdomen. This issue might be somewhat alleviated with the use of bariatric length telescopes. Longer laparoscopes can make it possible for the camera operator to hold the laparoscope further back and to leave the space closer to the access device for the surgeon to operate the instruments. Another deviation from the standard technical operation of the laparoscope is the light cord assembly. Traditionally the light cord attaches to the laparoscope at a right angle, which makes the laparoscope three-dimensionally space occupying. Assembling the light cord via a 90-degree angle connector will make the light cord and camera parallel, thus adding free space near the access device and enhancing the surgeon’s maneuverability to operate the surgical instruments.
9.3.2 Flexible Endoscope
Palanivelu et al. [21] were the first to describe the feasibility of flexible endoscope for performing single-port cholecystectomy in human patients. They used the endoscope’s working channels to pass instruments which assisted in the procedure. Soon after, more reports were published about a series of SPLS in both porcine models and in humans [11, 14, 22–23].
While definitely improving the compromised view of SPLS (due to both its ability to overlook the surgical field from multiple different angles and its inherent irrigation system), the use of a flexible endoscope has disadvantages as well. The lack of rigidity causes the endoscopes shaft to surender to the forces of gravity and hence often times the angle of view achieved is from down-up instead of the standard view. Most surgeons do not have experience with the flexible endoscope (gastroscope) and operating with this tool in the abdominal cavity is a new challenge that needs to be mastered. Another problematic issue is the limited availability of this device in the OR and the need for collaboration and cordination with gastroenterologists.
9.3.3 Modified Laparoscopes
Several modifications for the “classic” rigid laparoscopes have been developed. These modifications attempt to provide improvements for the viewing capabilities.
Two examples for such modifications are the EndoCAMeleon™ (Karl Storz-Endoscope), a 10-mm rigid non articulating scope with adjustable viewing angle of 0° to 120° and the IDEAL EYES HD™ Articulating Laparoscope (Stryker, Kalamazoo, MI, USA), a 10-mm scope equipped with an articulating tip with an angle range of up to 100° of flexion in all directions.
One study evaluated the efficacy of semi-rigid laparoscopes used in extreme angles (to view the anterior pelvis trans-vaginally) [24]. The conclusion was that there was no obvious advantage gained by using the new laparoscopes. Another study has evaluated the Storz EndoCAMeleon™, the Olympus EndoEye™ and the Stryker IdealEye™. These articulating laparoscopes were compared using standard industry testing protocols for image resolution, distortion and color reproducibility and were concluded with conflicting results [25]. Their use, nevertheless has been shown to be feasible in several case series [26–29].
Articulating laparoscopes are important tools in SPLS, however they are still not the ideal solution for acquiring the best imaging necessary. Several experimental cameras aimed toward achieving better viewing angles in SPLS are being developed. One experimental method of achieving enhanced visualization in SPLS, either as the primary camera or as an adjunct is the use of a miniature camera anchored to a laparoscopic articulating instrument (Fig. 9.7). This camera is still under development and holds the promise of having the ability to acquire additional angles of view during SPLS [30].
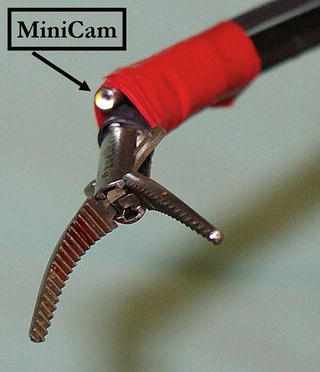
Fig. 9.7
A miniature camera anchored to a laparoscopic articulating instrument has the ability to supply additional angles for optimizing the view during SPLS
9.4 Retraction
One of the basic requirements of any kind of surgery is retraction. Retraction enables the surgical field to be visible to the surgeons in both open and laparoscopic surgery and enhances surgical dissection. As procedures become less invasive, adequate retraction must often be sacrificed, as ports designated for retraction are invariably the first to be waived. Nevertheless, surgeons must find ways to provide adequate retraction even though they use a reduced number of ports. Inadequate retraction undoubtedly serves as an obstacle when performing SPLS, especially when the anatomy encountered is less than “textbook” [31]. Aside from its inevitable prolongation of operative time, inadequate retraction can potentially convert a technically straightforward case into a complex ordeal, lead to the conversion of a single-port surgical procedure to conventional laparoscopy or open surgery, and eventually increase morbidity. As such, the achievement of optimal retraction without additional ports is an everlasting pursuit.
9.4.1 Trans-Abdominal Stay Sutures and Endoloops
One commonly employed method of retraction in SPLS is trans-abdominal stay sutures [32]. The sutures can be placed through the dissected organ (e.g. through the fundus of the gallbladder in cholecystectomy) using a straight Keith needle and then externalized trans-abdominal to allow continuous extracorporeal manipulation. This method allows for continuous external manipulation of the target organ while leaving a negligible mark where the needle passed through the skin. Some surgeons perform a variation of this method whereby the needle enters and exits the abdomen in two different locations (e.g. enters at the subxiphoid region, is sutured to the Hartman’s pouch and exits in the right lower quadrant) thereby enabling a “marionette” effect of external manipulation.
The major limitation of the trans-abdominal stay suture method of retraction is the potential perforation and leakage of gastrointestinal content into the peritoneal cavity; hence it is limited to surgeries which involve retraction of organs to be removed, e.g. cholecystectomy. Another drawback of this method is its restricted retraction capability, with a fixed anchoring point, which makes repositioning during surgery impossible.
Trans-abdominal endoloops have also been used to achieve gallbladder retraction during SPLS cholecystectomy [31, 33]. The endoloop is introduced trans-abdominally into the peritoneal cavity and is attached to the gallbladder, which is then retracted to the anterior abdominal wall. Endoloops are safer to use then stay sutures in the manner that they have less of a potential for a perforation or leak, given that they do not pierce the tissue. Nevertheless, their retraction capability is sub-optimal.
9.4.2 Magnetic Anchoring and Guidance System (MAGS)
Magnetic Anchoring and Guidance System (MAGS) employs intra-abdominal magnetically-anchored instruments to perform trocar-sparing laparoscopic surgery. MAGS uses 2 internal neodymium-iron-boron magnetic platforms introduced into the abdomen through a 12-mm trocar. The internal platforms are magnetically anchored to external anchors on the patient’s skin, capable of manipulating and stabilizing these platforms [34]. The internal magnetic platforms allow for a non-traumatic elevation and retraction of organs like the liver and spleen. A modification of the MAGS retraction system was described using magnet-conjugated clips, which were placed along the inferior edge of the liver and were used to accomplish retraction [35]. MAGS platform has recently also been described to operate surgical instruments and this way to enhance triangulation [36, 37]. Nevertheless, studies with the MAGS have only been performed on animal models and cadavers. The main technical pitfall of the MAGS system (in addition to its cost) is the exponential decrease in magnetic coupling strength as a function of distance (i.e. abdominal wall thickness). Hence, a tissue thickness greater than 15-mm does not allow use of the magnetic anchoring system [34].
9.4.3 Internal Retractors
The decreased ability to achieve optimal retraction in SPLS has led to the development of newly designed internal retractors. These devices are introduced to the abdominal cavity via the SPLS access system and anchor the target organ to the abdominal wall. An example for such a retractor is the EndoGrab™ (Virtual Ports Ltd., Caesaera, Israel) (Fig. 9.8) [14, 31]. This is an internally-anchored retracting device which can be introduced into the abdomen through a 5-mm port. Once deployed, one of the two grasping ends is attached to the target organ and the other is then anchored to the abdominal wall. Internal retractors can be anchored in different places within the abdominal cavity, including under the diaphragm without concern of entering the thoracic cavity. In addition, their position can be repeatedly adjusted throughout surgery in order to allow for a dynamic retraction, just like in open surgery. The ability of internal retractors to accomplish complete anterior-superior retraction of the gallbladder fundus was shown to be a distinct advantage over other methods [31].
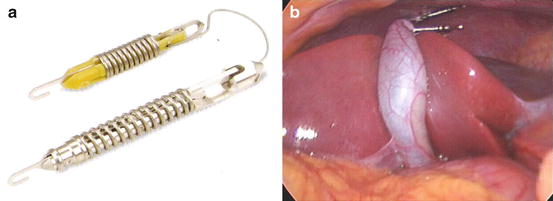
Fig. 9.8
(a) Endograb™ (Virtual Ports). The use of endo-retractors optimizes retraction and exposure capability including changing retraction angles during the operation. (b) Gallbladder retraction achieved with the device
9.5 Instruments
Traditional laparoscopic instruments are straight and rigid. The mobility of straight instruments is limited and when a few straight instruments are inserted through a common entry point in the abdominal wall, their maneuverability is lacking. In addition, in these circumstances triangulation of the instruments and camera towards the surgical field is limited as well, which turns even a simple surgical procedure into a technically demanding ordeal. This problem is even more prominent if the single-port access device is bulky and long [20]. Many efforts have been made to develop instruments that would simplify the technical challenge and would achieve triangulation, mainly curved and articulating instruments. Even though the use of straight laparoscopic instruments comes with technical difficulty, all laparoscopic instruments can still be used for SPLS. The main pros for the use of straight (“conventional”) laparoscopic instruments is the reduced cost associated with their use by eliminating the need to buy new instruments, and the elimination of a learning curve for the use of a new type of instruments [38]. Some studies have shown the feasibility and safety of large series of SPLS using standard laparoscopic instruments [38, 39].
9.5.1 Articulating Instruments
Articulating (also called “roticulating” or “wristed”) instruments are ones with maneuverability at their tip that can be controlled with movement of the surgeon’s wrist. Some of them allow locking of the articulation at the desired angle as well as 360° rotation of the tip (which when combined with the tip’s angulation creates a three-dimensional tip movement). The use of articulating instruments facilitates triangulation towards the surgical field and hence enhances the view and dissection capability (Fig. 9.9).
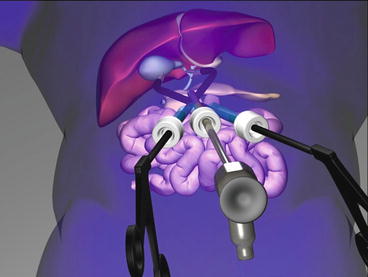
Fig. 9.9




Illustration of the need for triangulation, and the way to achieve it in SPLS surgery. Articulating instruments use enhances triangulation hence improving the view
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
