Chapter 19 Diagnostic angiography in hepatobiliary and pancreatic disease
Indications
Imaging Overview
In the 1980s and 1990s, selective angiography was commonly used as a diagnostic and staging technique. Indications would include ascertaining the organ of origin of an abdominal mass, assessing for vascular invasion by pancreatic or cholangiocarcinoma, and preoperative planning prior to hepatic resection. CT (see Chapter 16) and MRI (see Chapter 17) have completely replaced catheter angiography for these indications. In a prior edition of this book published in 2000, it was suggested that catheter angiography was a dying specialty and that angiographers should accept their fate with grace. However, a new age has dawned, and the volume of selective visceral angiography has increased considerably. The majority of these arteriograms are performed for the purpose of a diagnostic assessment prior to performing catheter-based interventions including radioembolizations (see Chapter 84A), chemoembolizations (see Chapter 83), chemoperfusions (see Chapters 86 and 89), and embolizations of bleeding arteries (see Chapter 25). In addition, endovascular therapies have replaced open surgical arterial interventions in patients with primary vascular pathology using angioplasties, stents, and the placement of stent grafts.
Arteries
Arteriographic Anatomy
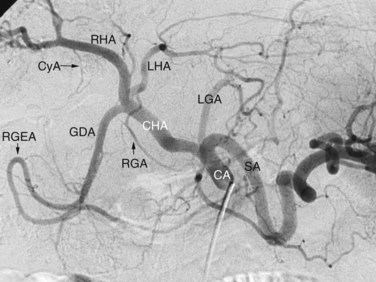
Arterial anatomy has been discussed elsewhere (see Chapter 1A, Chapter 1B ) and will only be briefly reviewed here. The most frequently encountered anatomy (Fig. 19.1) is the left gastric artery, splenic artery (SA), and common hepatic artery (HA) taking origin from the celiac axis. The common HA divides into the gastroduodenal artery (GDA) and proper HA, with the latter dividing into the right and left hepatic arteries. The right gastric artery most often originates from the base of the left HA, and the cystic artery most often originates from the right HA, but considerable variations in the origins of these arteries exist. Moreover, accessory duodenal arteries, either representing a supraduodenal or a retroduodenal artery, are frequently encountered; this is critical to recognize when planning chemoembolization and radioembolization.
The normal arterial supply to the liver is shown in Figure 19.2 (see the Extrahepatic Vasculature section in Chapter 1B), which shows the commonly recognized variations of the left hepatice artery (LHA), taking origin from the left gastric artery, and the right hepatic artery (RHA), taking origin from the superior mesenteric artery (SMA). It is important to recognize that either a part or the entirety of the right and left hepatic arteries may have these variant origins. When the entire vessel has a variant origin, it is termed replaced. If the entire trunk does not take a variant origin, the vessel is termed accessory. For example, if the right lobe is supplied by a right HA originating from the common HA, as well as a right HA taking origin from the SMA, the latter would be termed an accessory right HA. If the entire right lobe was supplied by an artery taking origin from the SMA, it would be called a replaced right HA.

The RHA conventionally divides into an anterior (ventral) and posterior (dorsal) branch. The anterior branch usually is more vertically oriented and supplies segments V and VIII. The posterior branch is usually more horizontally oriented and supplies segments VI and VII. More than one projection is usually required to ascertain with certainty which is the anterior branch and which is the posterior branch. In the right anterior oblique projection, the anterior branch moves medially and the posterior branch moves laterally when compared with the posteroanterior (PA) projection. The entire segmental arterial supply to the liver should be accounted for prior to hepatic arterial therapy, major hepatic resection, partial hepatectomy, or living-donor liver transplantation (LDLT, see Chapter 98B).
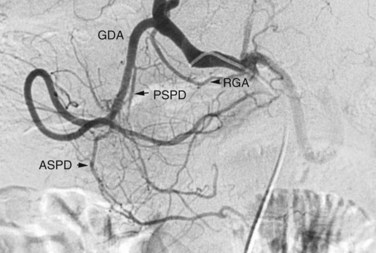
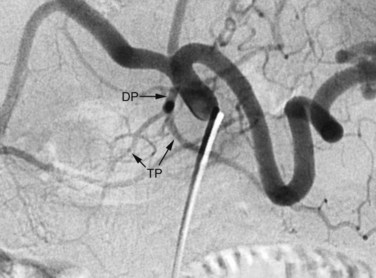
The arterial supply to the pancreas is somewhat variable. The most consistent supply is to the pancreatic head, afforded by an arcade formed by the inferior pancreaticoduodenal (IPD) branch of the SMA to the anterior superior and posterior superior pancreaticoduodenal branches of the GDA (Fig. 19.3). The transverse pancreatic artery runs along the middle portion of the long axis of the pancreas and may take origin from the arterial arcade in the head of the pancreas, directly from the GDA, or as a branch of the dorsal pancreatic artery, which variably originates from the common HA or SA (Fig. 19.4). A number of small branches from the SA supply the pancreatic body and tail, but the number and location of these arteries vary and must be identified in each individual patient when clinically relevant.
Preoperative Angiography: Historical Perspective
Prior to the advent of multidetector computed tomography angiography (MDCTA), visceral angiography was performed to assess the resectability of pancreatic and biliary tract tumors by demonstrating the presence or absence of vascular invasion. The sensitivity of catheter angiography for this purpose was low, and MDCTA has replaced catheter angiography for this indication. Using angiography for diagnosis of a hepatic mass, such as differentiating a cavernous hemangioma from a hepatocellular carcinoma, is no longer performed, as no improvement in diagnostic accuracy can be achieved over conventional cross-sectional imaging techniques (see Chapters 16 and 17).
Arteriography in Conjunction with Arterial Interventions
Accurate delineation of arterial anatomy has increased in importance remarkably as radioembolization (see Chapter 84A) and chemoembolization (see Chapter 83) have gained widespread application. The inadvertent administration of radiation or chemotherapeutic agents into arteries supplying the stomach or duodenum can lead to significant adverse outcomes. When performing procedures designed to necrose tumor, it is imperative that normal structures be spared. To accomplish this, variant anatomy must be recognized. The importance of accessory branches to the duodenum, including the supraduodenal and retroduodenal arteries, is now well known. Communications from intrahepatic branches to the lower esophagus, stomach, and diaphragm are of equal importance (Miyayama et al, 2009; Liu et al, 2005).
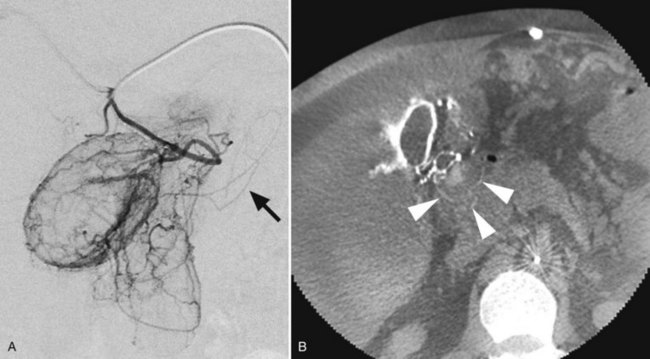
With current angiographic technology, it is possible to obtain a volumetric digital image during the arterial injection of contrast media and to display the images in a computerized tomographic format (i.e., C-arm CT) (Wallace et al, 2008). Using this technique it is possible to identify extrahepatic perfusion from aberrant hepatic arterial branches that may be unrecognized on the basis of the angiogram alone (Fig. 19.5).
Hemorrhage
Splenic Bleeding
The most common cause of bleeding from the spleen is blunt trauma, and nonoperative management is currently the standard of practice. SA embolization has been established as a method to increase the success rate of nonoperative management of traumatic splenic injuries (Dent et al, 2004). A comparative study between two cohorts consisting of 625 patients over a 15-year period revealed an improved success rate of nonoperative management from 77% to 96% with the advent of splenic embolization (Rajani et al, 2006). The indications for splenic arteriography and splenic arterial embolization are based upon CT findings and include active contrast extravasation, splenic vascular injuries, and significant hemoperitoneum. Moreover, the American Association for the Surgery of Trauma recommends angiography for grade III, IV, and V splenic injuries (Raikhlin et al, 2008).
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


