Fig. 2.1
Co-axial setup. Monitor, surgical field, camera port, and the operator are ideally placed in a line
Fig. 2.2
Triangular formation. Instruments from both sides should make an angle of 30° to 60° to the line (axis) mentioned above
In SLS, the ports for scope and instruments are placed in a restricted area, the angles between the scope and instruments are less than 10° at the surgical site. The principle of triangular formation is violated, which imposes problems that are not usual in standard laparoscopic surgery.
The shaft of the instruments and the scope interfere with each other (“sword fighting”). In standard laparoscopic surgery, the length of the instruments is uniformly 33–35 cm. This fact adds clashing problems, in which the handles of instruments interfere with each other outside the abdomen. The relatively large housing of regular ports also clash. In addition, the light guide in a rigid angled scope and the camera head further complicate this clashing problem. Furthermore, the shaft of the instruments tends to eclipse the surgical field for this narrow angle, making it difficult to see the exact place where the force and energy is applied (Fig. 2.3) [16].

Fig. 2.3
Eclipse of the surgical field. Because of the narrow angle between the scope and instrument, the shaft of the instrument tends to eclipse the surgical site where the force and energy is applied
2.4 Instrumentation and Techniques in SLS
Regardless of the names, including SILSTM (Single-Incision Laparoscopic Surgery, Covidien http://www.covidien.com/), LESSTM (Laparo-Endoscopic Single-Site surgery, Olympus http://www.olympusamerica.com/LESS/, http://www.advancedsurgical.ie/), SSLTM (Single Site Laparoscopy J&J http://www.jnj.com/connect/), and S-PortalTM (Karl Storz Endoskope, http://www.karlstorz.com/cps/rde/xchg/karlstorz-en/hs.xsl/146.htm), the underlying concept is almost identical, restoration of triangular formation while avoiding clash and “sword fighting.” In order to restore triangular formation, two basic techniques have been employed, first placing the operating ports at a good distance of separation from one another, and second using curved, angulated, or articulated instruments. The first technique is commonly referred to as the parallel technique, and the second one as the cross hand technique (Figs. 2.4 and 2.5). In clinical settings, these techniques are often in mixed use. Tissue retraction is a key step of operation for good exposure of the surgical field with some tension to apply force and energy to the surgical site. In standard laparoscopic surgery, the assisting forceps is inserted through an independent port to achieve this. In SLS, additional instruments from the same wound further complicate the clashing problem. Sutures are introduced in the abdominal cavity from a different site and the tissue is pierced, and then the sutures are retrieved through the abdominal wall. By pulling the thread outside, the tissue is retracted. Although some surgeons advocate this technique, it is cumbersome and sometimes causes bile spillage in laparoscopic cholecystectomy. Gadgets that measure 1.6–3 mm in caliber, including pre-tied loop, wire snare, and a needle grasper can be independently inserted elsewhere as in standard laparoscopic operations and used for tissue retraction (Fig. 2.6). The use of additional instruments adds confusion to the terminology of SLS, because these techniques leave an additional wound, even though small and in name, scarless. The purists of SLS demanded that these techniques requiring another wound should be distinguished from the pure one, resulting in further confusion of the terminology including with one additional port surgery, single plus one port laparoscopic surgery, or two-port laparoscopic surgery [19–21].
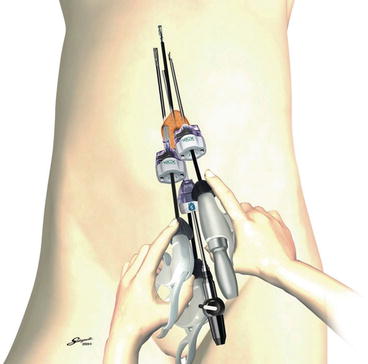
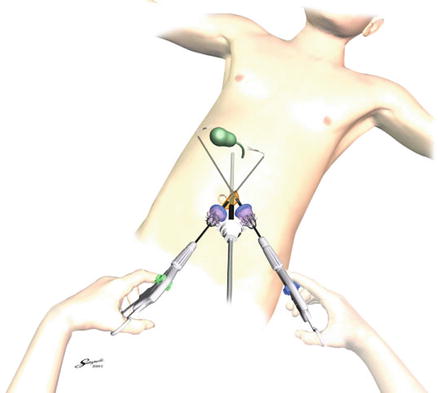
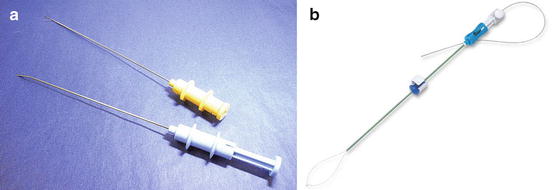
Fig. 2.4
Parallel Technique (Boxing Style). In parallel technique, the operating ports are placed at a distance of 1.5–2.5 cm away from the scope port
Fig. 2.5
Cross Hand Technique. In the cross hand technique, the shafts of the instrument cross at some point and the instrument that approaches the surgical site from the left-side is manipulated by the right hand
Fig. 2.6
Gadgets for Tissue Retraction. (a) Riza-Ribe Needle and GraNee Needle (M-Med). (b) Mini loop retractor (Covidien)
2.5 Needle-Scopic Surgery
Although the term needle-scopic surgery was first used in 1996 by Mathias [22], Tanaka in 1997 is usually credited with the first report of needle-scopic cholecystectomy in humans [10]. This report was followed by a number of clinical reports from various fields of surgery [23–25]. The merits of needle-scopic surgery included its cosmetic advantage over standard laparoscopic surgery while keeping the operability of instruments. Several randomized control studies were conducted, but failed to prove the better outcome of needle-scopic cholecystectomy when compared to standard laparoscopic cholecystectomy in regard to postoperative pain, convalescence and recovery [26–28]. The disadvantages of needle-scopic surgery result from the small caliber of the scope and instruments. The image that needle-scope provides is unsatisfactory. The shaft of the forceps bends when force is applied, and the small jaws of instruments tend to bite the organs more easily than atraumatically-designed jaws of standard laparoscopic instruments.
In a meta-analysis by Sajid et al. [29], needle-scopic cholecystectomy was reportedly associated with longer operating time and higher conversion rate comparing to standard laparoscopic cholecystectomy. Although needle-scopic surgery has been routinely performed for relatively simple procedures in pioneering institutions, it failed to gain wide acceptance as a standard procedure to date.
2.6 Inception of Reduced Port Laparoscopic Surgery (RPLS)
In general, SLS is more technically demanding than standard laparoscopic surgery. In the beginning, indications suggested that it was limited to relatively simple operations. Many surgeons have noticed that the pros and cons that SLS and needle-scopic surgery bring are complementary to each other and the mixed use of two techniques drastically mitigate difficulties in SLS. Surgeons started using needle instruments as an active forceps [30]. These approaches are collectively called RPLS. Unleashed from the limitations of SLS, RPLS widened its indication to a variety of procedures, as is described in this book. Interestingly, the introduction of RPLS evoked the idea of hybrid use of other approaches of minimally invasive surgery, including robotic surgery and NOTES [31, 32]. The daVinci single-site platform (Intuitive Surgical Inc., Sunnyvale, CA, USA) is already on the market (Fig. 2.7), and endoscopic robot designed for NOTES was introduced through an access device of SLS. A flexible endoscope is also introduced through the single access device, and the endoscopic device through the working channel is used as a forceps in cooperation with standard instruments [33]. Assisting forceps were reportedly introduced through the port placed in the vagina, and the specimen was eventually retrieved via the vagina [34]. Various approaches to minimize invasiveness of surgery merge here in reduced port laparoscopic surgery. In the toolbox of RPLS, we have a wide variety of tools, including standard and needle-scopic instruments, robots, NOTES devices, and even the flexible endoscope and its various forceps (Fig. 2.8).










