Fig. 16.1
Port arrangements. Left: Port arrangement for cholecystectomy. A 12-mm port is inserted via open approach at the umbilicus. A 5-mm port is below the left costal margin (OP). Two puncture sites with a 2-mm port are below the right costal margin on the mid-clavicular line (MC) and on the right anterior-axillary line of the navel level (AA). Middle: Arrangement for transcystic duct exploration. The MC port is changed to a 3-mm port for exploration. Right: In the arrangement for trans-choledochal exploration (LCHE), a 5-mm port is added at the subxiphoid level. When LCHE is clearly supposed to apply preoperatively, the MC port will be arranged as 3-mm
Although some say that the cases with recent previous abdominal operations should be excluded, but it is worth trying even after LC. Those with Mirizzi’s syndrome, cicatrice change of Calot’s triangle, confluence stone and atrophic gallbladder are not suitable for needlescopic LCBDE, but it may depend on the surgeon’s skill.
16.3 Description of the Technique
16.3.1 Port Arrangement and Needle Equipment
LCBDE is usually performed with LC. Unless the patient has been proven suitable for LCHE preoperatively, indication of LCBDE should be decided during intraoperative cholangiography (IOC), according to the size and number of the stones. The port arrangement is identical to those in needlescopic-LC (N-LC), consisting of two punctures and two incisions (Fig. 16.1). The primary surgeon stands on the patient’s left side, with the assistant on the patient’s right. Initial entry into the abdomen is made via an open approach at the umbilicus. Typically, a 12-mm port is inserted at this location. Another incision is made below the left costal margin for the 5-mm port (OP). The puncture sites are below the right costal margin on the mid-clavicular line (MC) and on the right anterior-axillary line of the navel level (AA). Two-millimeter forceps are inserted through these thin caliber ports (Fig. 16.2). We used ‘BJ needle’ (Niti-On Company, Tokyo, Japan) or ‘Mini-Site’ (Covidien, New Haven, CT, USA) as 2-mm forceps. These forceps can be inserted through the thin caliber trocar ‘Mini-Port’ (Covidien, New Haven, CT, USA) by puncture without incision. Because Mini-Site (Covidien) was discontinued, we have mainly used BJ needle (Niti-On) in recent years. Fig. 16.3 shows the set up for a N-LC. For both N-LC and LCBDE procedures, a 30°, 10-mm laparoscope is introduced through the umbilical port. The MC port is used for retracting and manipulating the gallbladder and the liver with a BJ needle (Niti-On) by the assistant. The primary surgeon uses the OP and the AA ports. A 5-mm titanium clip, a 5-mm energy device, such as electrical cautery and laparoscopic ultrasonic coagulating shears (LCS), or 5-mm scissors are introduced through the OP port. We routinely perform IOC using Urographine (Bayer Yakuhin, Osaka, Japan) diluted with saline by 30 % with an introducing catheter via the MC. The catheter for IOC is LAP-13 (Ranfac, Avon, MA, USA), Cholagiocatheter TH type (Hakko-medical, Tokyo, Japan), or thin caliber (2-mm) feeding tube (atom tube, Atom Medical, Tokyo, Japan).
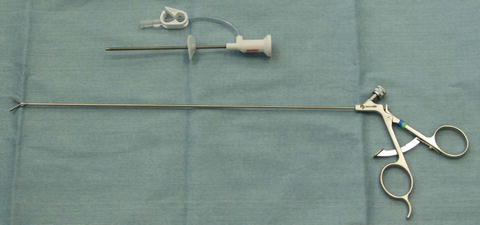
Fig. 16.2
Two-millimeter needle forceps and port
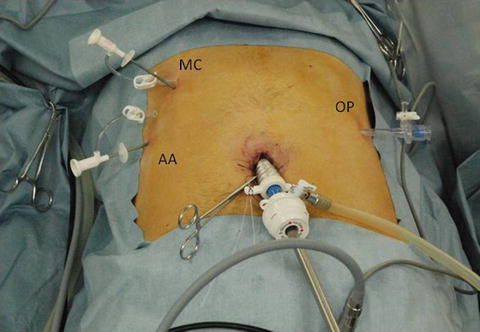
Fig. 16.3
Port set up for needlescopic cholecystectomy
With the confirmation of CBDs with IOC, LCBDE is performed followed by cholecystectomy.
16.3.2 LTCE with Needle Forceps
Following IOC, the route of LCBDE is decided according to the condition of CBDs (Fig. 16.4). When the number of stones is 4 or less and within 8-mm in diameter, the case will be suitable for LTCE (Table 16.1).

Fig. 16.4
Indications of approaches to common bile duct according to intraoperative cholangiography. Left: One small stone (arrow) is observed at the end of common bile duct. This is for trans-cystic duct exploration. Right: Stones more than 8-mm in diameter (arrows) are for the choledochal approach
Table 16.1
Indications of approach for common bile duct exploration
LTCE | LCHE | |
|---|---|---|
Conditions of stones | ||
Number | ≦4 | 5< |
Size | <8 mm | 8 mm≦ |
Others | Unsuitable for LTCE | |
At the beginning of LTCE, the MC port is changed to 3-mm for exploration, and the grasper through the AA port is fixed to hold the tail of the gallbladder (Fig. 16.1).
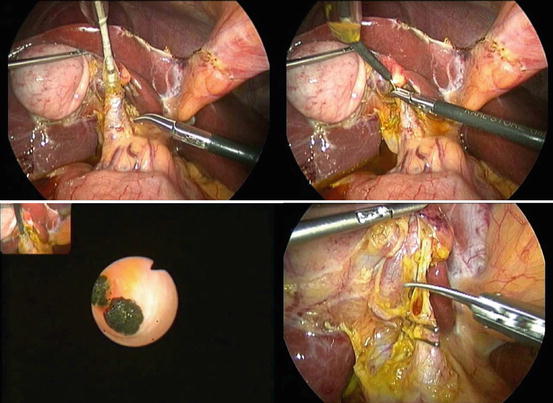
The atom tube from the MC port is cannulated in the cystic duct about 5-cm long. Then the guide wire (0.035-mm in diameter) is inserted into the common bile duct (CBD) through the atom tube, but not through it. The atom tube is removed, leaving the guide wire, and a 6Fr balloon catheter (Ascend AQ balloon catheter, Cook Japan, Tokyo, Japan) is then inserted over the guide wire. The balloon is gradually inflated until it reaches 6-mm in diameter with an atmospheric pressure of 13. After 4 min, the balloon is deflated and removed, leaving the guide wire, and a 2.8-mm cholangioscope (CHF-CB30S, Olympus, Tokyo, Japan) is inserted over the guide wire. Under the cholangioscope vision, the stones are removed via the cystic duct using 3.2Fr basket catheter (Fig. 16.5).