CHAPTER 122 Colonic Polyps and Polyposis Syndromes
COLONIC POLYPS
Colonic polyps may be divided into two major groups: neoplastic (the adenomas and carcinomas) and non-neoplastic (Table 122-1). The adenomas and carcinomas share a characteristic—cellular dysplasia—but they may be subdivided according to the relative contribution of certain microscopic features. The non-neoplastic polyps may be grouped into several distinct categories: hyperplastic polyps (including serrated polyps), “mucosal polyps,” juvenile polyps, Peutz-Jeghers polyps, inflammatory polyps, and others. Submucosal lesions also can impart a polypoid appearance to the overlying mucosa and therefore are briefly mentioned even though they are not true polyps.
Table 122-1 Classification of Colorectal Polyps
| Neoplastic Mucosal Polyps |
| Benign (Adenoma) |
| Malignant (Carcinoma) |
| Non-Neoplastic Mucosal Polyps |
| Submucosal Lesions |
NEOPLASTIC POLYPS
Pathology
Histologic Features
Adenomatous polyps are tumors of benign neoplastic epithelium that can either be pedunculated (i.e., attached by a stalk) or sessile (i.e., attached by a broad base with little or no stalk). The neoplastic nature of adenomas is apparent by histologic examination of their glandular architecture. Tubular adenomas are the most common subgroup and are characterized by a complex network of branching adenomatous glands (Fig. 122-1A). In villous adenomas, the adenomatous glands extend straight down from the surface to the center of the polyp, thereby creating long, finger-like projections (see Fig. 122-1B). Tubulovillous (villoglandular) adenomas manifest a combination of these two histologic types.
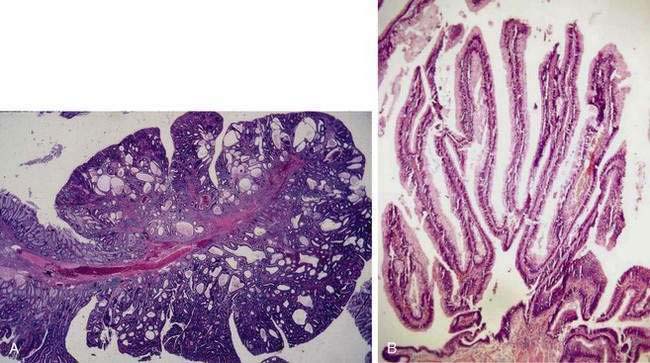
A polyp is assigned a histologic type on the basis of its predominant glandular pattern, and in practice, pure villous adenomas are quite rare. According to the World Health Organization, adenomas are classified as tubular if at least 80% of the glands are of the branching, tubule type and as villous if at least 80% of the glands are villiform.1 Of all adenomatous polyps, tubular adenomas account for 80% to 86%, tubulovillous for 8% to 16%, and villous adenomas for 3% to 16%.2,3 Tubular adenomas usually are small and exhibit mild dysplasia, whereas villous architecture is more often encountered in large adenomas and tends to be associated with more severe degrees of dysplasia (Table 122-2).

The dysplasia exhibited by all adenomas can be graded subjectively on the basis of certain cytologic and architectural features into three categories: mild, moderate, and severe. Some polyps contain the entire spectrum from mild to severe dysplasia, but in all cases, the adenoma is classified according to its most dysplastic focus. In cells that exhibit mild dysplasia, the nuclei in the cell maintain their basal polarity but are hyperchromatic, slightly enlarged, and elongated, yet uniform in size, without prominent nucleoli (Fig. 122-2A). There often is loss of goblet cell mucin. Architecturally, the glands manifest branching and budding and become more crowded. With moderate dysplasia, nuclei become stratified and pleomorphic, with prominent nucleoli, along with further loss of goblet cell mucin and increased glandular crowding. Severe dysplasia (see Fig. 122-2B) is characterized by further stratification and pleomorphism of nuclei, more numerous and prominent nucleoli, increased nucleus-to-cytoplasm ratios, and extreme glandular crowding.
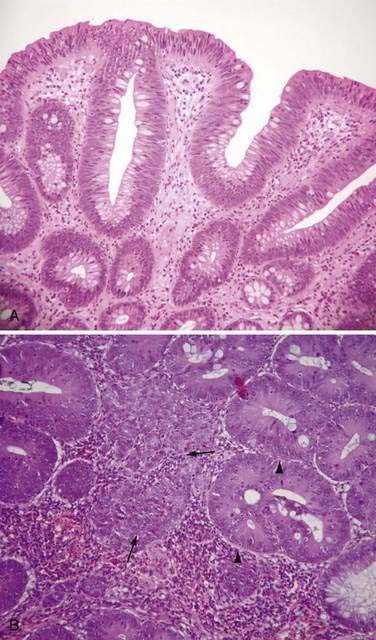
With further cell proliferation within the crypt, cells pile up, lose polarity, and create glands within glands, giving a disorderly cribriform appearance termed carcinoma in situ (see Fig. 122-2B). Most pathologists group severe dysplasia and carcinoma in situ, considering them both high-grade dysplasia2; one reason for this grouping is to avoid using the term carcinoma for these lesions because they often can be managed endoscopically rather than surgically (see later). Indeed, it is now common practice to categorize dysplasia in colorectal adenomas into only two grades: low-grade dysplasia, which includes mild and moderate dysplasia, and high-grade dysplasia, which comprises severe dysplasia and carcinoma in situ.
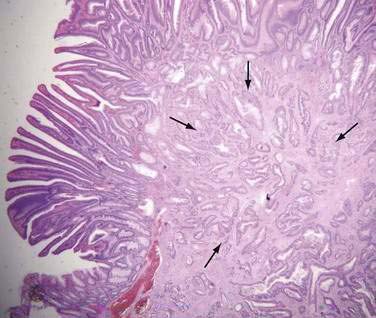
Carcinoma in situ is characterized by intracryptal cell proliferation that leaves intact the basement membrane surrounding the gland. If a focus of neoplastic cells grows beyond the basement membrane and into the lamina propria of the mucosa, the lesion is termed intramucosal carcinoma (see Fig. 122-2B). Both carcinoma in situ and intramucosal carcinoma are noninvasive lesions without metastatic potential, because lymphatics are not present in the colonic mucosa above the level of the muscularis mucosae.4 Because clinical confusion often arises on encountering these two entities, it has been suggested that both carcinoma in situ and intramucosal carcinoma be reported as “noninvasive carcinoma” to avoid unnecessarily aggressive management. Only when a focus of neoplastic cells has spread through the muscularis mucosae is the lesion considered invasive carcinoma (Fig. 122-3). An adenoma that contains a focus of invasive carcinoma commonly is referred to as a malignant polyp (see later).
Of all adenomatous polyps, mild dysplasia is found in 70% to 86% moderate dysplasia in 18% to 20%, severe dysplasia (carcinoma in situ) in 5% to 10%, and invasive carcinoma in 5% to 7%.3,5,6 Higher grades of dysplasia are more common in adenomas of larger size and greater villous content,2 and adenomas with severe dysplasia are more likely to contain foci of invasive cancer.
Adenoma Size
Adenomas are categorized into three size groups: less than 1 cm, 1 to 2 cm, and greater than 2 cm.5 Overall, most adenomas are smaller than 1 cm, but the size distribution of adenomas can vary greatly among studies, depending on study design, age of the study population, and location of the adenomas within the colon. Thus, in autopsy series, which describe a presumably asymptomatic population dying of other causes, only 13% to 16% of adenomas are larger than 1 cm,7–9 whereas surgical and colonoscopic series that include symptomatic or higher-risk patients report a higher prevalence (26% to 40%) of adenomas larger than 1 cm.2,3,5 In countries where the prevalence of colon cancer is high, adenomas tend to be larger than in low-prevalence countries.10,11 Adenoma size increases as a function of age,8,12,13 even in low-prevalence countries,10 and larger adenomas are more common in distal colonic segments.2,5,8
Diminutive Polyps
Diminutive polyps measure 5 mm or less in diameter and are commonly encountered during endoscopy. An earlier concept that these lesions were almost always non-neoplastic has been revised based on several flexible sigmoidoscopic and colonoscopic studies in which 30% to 50% of diminutive polyps were found to be adenomatous14–18; despite the frequency of adenomatous change, however, they represent little if any threat of cancer. Earlier studies found that less than 1% of diminutive polyps were villous or contained a focus of severe dysplasia and that they almost never harbored invasive carcinoma.14–16,18 In an analysis of 4381 diminutive polyps, 4.4% contained severe dysplasia or villous components, although still only 0.1% had invasive carcinoma.19 Moreover, in a retrospective study of predominantly asymptomatic people with diminutive adenomas found on flexible sigmoidoscopy, full colonoscopy identified a synchronous proximal adenoma in only 33% of subjects, and most of the proximal lesions were smaller than 5 mm.20 Likewise, prospective colonoscopic studies confirm only a 24% to 34% prevalence of proximal adenomas in asymptomatic patients with distal diminutive polyps (of all histologic types)21,22; the likelihood of finding proximal adenomas is greater when the distal polyp is larger than 5 mm.21 Diminutive adenomas manifest little, if any, appreciable growth over time.23,24 A population-based study that involved fulgurating small polyps (even those up to 1 cm) without obtaining initial histologic identification reported that the subsequent risk for colorectal cancer and overall survival was no worse than in the general population.25
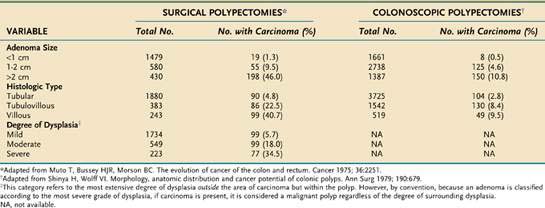
Malignant Potential of Adenomatous Polyps
The three principal features that correlate with malignant potential for an adenomatous polyp are size, histologic type, and degree of dysplasia (Table 122-3). Although higher rates of malignant transformation are found when the source of the pathologic material is mainly from surgical polypectomies5 rather than colonoscopic polypectomies,6 the malignant potential is correlated directly with larger adenoma size, more villous histology, and higher degrees of dysplasia. These three histopathologic criteria usually are interdependent, so it is difficult to assign a primary premalignant role to any one of them. For example, although only 1.3% of all adenomas smaller than 1 cm harbor a cancer (see Table 122-3), if these small lesions have a predominant villous component or contain a focus of severe dysplasia, the cancer rate rises to 10% or 27%, respectively (Table 122-4). A small (<1 cm), tubular, mildly dysplastic adenoma is highly unlikely to harbor a focus of invasive cancer. Nonetheless, although this type of lesion is innocuous in itself, once removed, it often is considered a marker of a person who is at (low) risk for developing a recurrent adenoma (discussed later). Because adenomas that are larger than 1 cm, have villous architecture, or manifest high-grade dysplasia or carcinoma represent a more biologically hazardous group, the term adenoma with advanced pathology (AAP) often is applied to adenomas that display any of these features.

Other Adenoma Variants
Flat Adenomas
A subset of adenomas, termed flat adenomas by Muto and coworkers,26 is receiving increasing attention as a potentially important lesion. Macroscopically, a flat adenoma is either completely flat or slightly raised and can contain a central depression. By definition of the Japanese Society for Cancer of the Colon and Rectum, the diameter of this polyp is more than twice its thickness. Typically smaller than 1 cm in diameter, these lesions can be easily missed at endoscopy. This potential risk has prompted investigators, particularly in Japan, to adapt better methods of detection that involve dye-spraying (chromoendoscopy) to generate a contrast relief-map image of the mucosa, or magnification colonoscopy, for enhanced visualization.27 In studies without such specialized endoscopic techniques, flat adenomas accounted for 8.5% to 12% of all adenomas and could be multiple.28
Prospective studies of Western populations aided by the use of chromoendoscopy found that 6.8% to 36% of all detected adenomas were flat. Compared with lesions that were polypoid, these flat polyps tended to be smaller and to have increased rates of high-grade dysplasia and early cancer.29–31 The largest study to date looked at over 1800 veterans undergoing colonoscopy. The prevalence of flat or nonpolypoid neoplasms was 9.4%. These lesions were 10 times more likely to harbor a carcinoma, although the rate of carcinoma was quite low.32 Indeed, it has been suggested that flat adenomas can have distinct biologic and chromosomal profiles.30,33 In contrast, re-evaluation of adenomas removed during the National Polyp Study found no increased risk of high-grade dysplasia in polyps classified as flat, based on histologic features.34 Future studies might help define whether broader acceptance of advanced endoscopic techniques such as chromoendoscopy or narrow-band imaging by endoscopists in Western countries will result in higher detection rates of flat adenomas, lower colorectal cancer incidence, or both following colonoscopy.35 A hereditary flat adenoma syndrome in four families described by Lynch and colleagues36 subsequently was confirmed to be a variant of familial adenomatous polyposis (FAP) (see later).
The natural history of flat adenomas is not known. It is possible that they give rise to typical polypoid adenomas. Alternatively, the facts that residual flat adenoma tissue can be found adjacent to flat carcinomas, that some studies have observed a substantial incidence of high-grade dysplasia in these small lesions, and that flat adenomas have a lower incidence of K-ras mutations compared with polypoid adenomas, suggest that malignant progression from flat adenomas might not necessarily involve a polypoid phase.37 It is possible that flat adenomas are the precursors of the long-recognized, but uncommon, small de novo colon carcinomas.38
Aberrant Crypts
Investigations of human and carcinogen-treated rat colonic mucosa have disclosed a putative preneoplastic lesion called the aberrant crypt.39 Found within macroscopically normal mucosa, aberrant crypts can occur individually or as small, slightly raised foci. They can be identified in methylene blue-stained whole mounts of colonic mucosa using a low-power lens or with a magnifying endoscope.40 When viewed from above, the lumina of aberrant crypts are elliptical and irregular rather than circular. Aberrant crypt foci have become useful biomarkers in animal studies of colon carcinogenesis and chemoprevention. Human aberrant crypts often are hyperplastic; however, when they are dysplastic, they can represent the earliest detectable preneoplastic lesions. This notion is supported by molecular studies indicating that dysplastic, but not hyperplastic, aberrant crypts manifest mutations in the adenomatous polyposis coli (APC) gene (see later).41
In one study, patients who had aberrant crypt foci in the rectum underwent repeat colonoscopy in one year42; at which time 60% of patients had aberrant crypt foci, but less than half had the same foci re-identified and 50% had new foci; this suggests that the progression of aberrant crypt foci is a dynamic process. In a large study using high-magnification chromoendoscopy to identify aberrant crypt foci in the rectum, the number of aberrant crypt foci increased in a stepwise fashion in normal patients, patients with a flat adenoma, and patients with a flat carcinoma.43 Despite these findings, it remains to be fully elucidated if aberrant crypt foci are useful biomarkers for adenomas.
Pathogenesis
Histogenesis
Adenomatous polyps are thought to arise from a failure in a step, or steps, of the normal process of cell proliferation and cell death (apoptosis). The initial aberration appears to arise in a single colonic crypt in which the proliferative compartment, instead of being confined to the crypt base, is expanded throughout the entire crypt. This disturbance results in a unicryptal adenoma. The DNA-synthesizing cells at the surface are not sloughed into the lumen, as normally occurs, and they accumulate in a downward infolding manner, interposing themselves between normal preexisting crypts. New adenomatous glands then are created either by further infolding or by branching. Thus, the unicryptal adenoma is believed to arise from a monoclonal expansion of an abnormal cell, and as the adenoma enlarges, the adenomatous cell population becomes polyclonal. Evidence for this concept comes from studying intestinal tissues from an extremely rare patient with FAP who was an XO/XY mosaic.44 Analysis of Y chromosome expression in the intestinal mucosa of this patient revealed that normal crypts of the small and large intestine and even unicryptal adenomas were monoclonal (either XO or XY), whereas at least 76% of very small microadenomas were polyclonal. Whether the same situation also applies to sporadic adenoma development is not clear at present.
Adenoma-Carcinoma Hypothesis
Epidemiologic Evidence
The prevalence of adenomas within a population, and the prevalence of people with multiple adenomas, geographically parallel the prevalence of colon cancer.10 Indeed, adenoma prevalence increases in migrants from low-risk to high-risk colon cancer regions (see Chapter 123). The prevalence rates for both adenomatous polyps and cancer increase with age, and age distribution curves indicate that the development of adenomas precedes that of carcinomas by 5 to 10 years.5,45
Clinicopathologic Evidence
The most compelling evidence for the adenoma-carcinoma sequence is the fact that in patients with FAP who have hundreds to thousands of adenomas, the development of colorectal cancer is inevitable. For persons in the general population without an inherited predisposition to colon cancer, perhaps the best evidence that adenomas give rise to carcinomas comes from endoscopic intervention studies. The National Polyp Study (see later) demonstrated that colonoscopic removal of adenomas results in a much lower than expected incidence of subsequent colorectal cancer.46 In addition, screening proctosigmoidoscopy can lower the expected incidence of47 and mortality from48 rectal cancer. Pathology-based studies often describe the presence of remnant adenoma tissue within colon cancers. Conversely, small foci of cancer are extremely rare in normal mucosa but commonly are found in adenomas, particularly in those that are larger, more dysplastic, and more highly composed of villous elements (see Tables 122-3 and 122-4). Furthermore, the site distribution within the colon is similar for large adenomas and colon cancers. In addition, adenomatous polyps are found in one third of surgical specimens that contain a single colon cancer and in more than two thirds of specimens that contain more than one synchronous cancer.
Molecular Genetic Evidence
Molecular genetic studies provide some of the strongest experimental support for the adenoma-carcinoma hypothesis. The progression from adenoma to carcinoma results from an accumulation of molecular genetic alterations involving, among other changes, activation of oncogenes, inactivation of tumor suppressor genes, and participation of stability genes (see Chapter 123).49 The K-ras oncogene commonly undergoes point mutations at particular sites within the gene, thereby endowing it with the ability to transform cells. Only 9% of small adenomas exhibit K-ras gene mutations, compared with 58% of adenomas larger than 1 cm and 47% of colon cancers50; therefore, K-ras activation can act at an intermediate stage in tumorigenesis, perhaps contributing to a polypoid growth pattern. The fact that a large number of adenomas and cancers do not have K-ras gene mutations indicates that other genetic events also must play a role.
Tumor suppressor genes that normally function to suppress tumor development commonly are inactivated in colorectal neoplasms by mutation or allelic deletion, thereby promoting tumorigenesis. The loss of function of tumor suppressor genes on chromosomes 5q, 18q, and 17p is critical for colorectal tumorigenesis. The APC (adenomatous polyposis coli) gene, which resides on the long arm of chromosome 5, is considered the gatekeeper for the process of colon carcinogenesis.51 Mutation or loss of this gene is believed to be the crucial first step that confers susceptibility to colonic adenomas in patients with FAP as well as in people with sporadic adenomas. The APC protein plays an important role in colonic epithelial cell homeostasis (see later). Other tumor suppressor genes are located on chromosome 18q, in a region where the DCC (deleted in colon cancer) gene resides. Loss of function of DCC, or other nearby tumor suppressor genes, seems to contribute to later stages of adenoma progression, because allelic deletion at this locus occurs in only 11% to 13% of small tubular or tubulovillous adenomas, but increases to 47% of adenomas with foci of cancer and 73% of frank colon cancers.52 Allelic deletion of chromosome 17p, at the locus that contains the TP53 gene, is the most common region of allelic loss in colorectal cancers. Because adenomas seldom manifest 17p deletion,52 this alteration probably occurs as a late step in the adenoma-carcinoma progression. Perhaps the most compelling molecular evidence that colon carcinomas arise from previous adenomas is that when cancer cells arise in a malignant adenoma, their pattern of molecular alterations is identical to that of the neighboring adenoma cells, but in addition, they have acquired further mutations that are presumably critical for malignant behavior.52
Oncogenes and tumor suppressor genes enhance the adenoma-carcinoma process by directly stimulating cell proliferation and inhibiting cell death; however, stability genes, or caretakers, normally keep genetic alterations to a minimum, and thus, when they are inactivated by mutation or loss, they permit mutations in other target genes to occur at a higher rate.49 Examples of stability genes include the DNA mismatch repair (MMR) and base-excision repair (BER) genes responsible for repairing subtle mistakes that are made during DNA replication. Germline mutations of DNA MMR genes (such as hMLH1, hMSH2, hMSH6) occur in persons with HNPCC, whereas inheritance of a mutated BER gene (e.g., MUTYH, also known as MYH) is responsible for a type of attenuated adenomatous polyposis (see later).
Pathways of Colon Carcinogenesis
It is useful to consider the process of colon carcinogenesis in two general stages: the formation of the adenoma, termed tumor initiation, and the progression of the adenoma to carcinoma, termed tumor progression (Fig. 122-4). It is believed that most, if not all, adenomas arise from an initial loss of APC gene function, and for that to happen, epithelial cells must lose the function of both APC alleles (two hits). In patients with FAP, one APC allele is inherited in a mutated form (germline mutation) from the affected parent. Adenomas arise when the second, normal copy of the APC gene from the unaffected parent either is lost or mutated (somatic mutation). Because persons with FAP are born with the first hit, they develop polyps at a much younger age and in much greater number than does the general population; thus, FAP can be considered a condition of accelerated tumor initiation. Despite this abnormal initiation rate, once adenomas form in patients with FAP, it is believed that each adenoma tends to display a normal progression to carcinoma. Thus, the inevitable progression to cancer in FAP is more a consequence of the numerous polyps than of any increased premalignant potential of the individual adenoma. In the general population, sporadic adenomas arise as a consequence of two acquired somatic mutations of the APC gene. Because two acquired hits are statistically less likely than one acquired hit, sporadic adenomas tend to occur later in life and to be fewer than the polyps in patients with FAP.
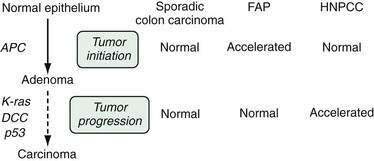
Another major molecular pathway for colon carcinogenesis involves mutations in DNA MMR genes (see Chapter 123); this is the predominant pathway in patients with HNPCC. Mutations in these enzymes result in a characteristic molecular phenotype termed microsatellite instability (MSI), a phenomenon that is observable in colon cancer cells from approximately 85% of HNPCC colon cancers but in only 15% of sporadic colon cancers. Although its name implies a lack of polyps, HNPCC colon cancers do arise from preexisting adenomas. It is believed that the numbers of adenomas that occur in patients with HNPCC are similar to those in the general population but that HNPCC is marked by an accelerated tumor progression stage, so the few adenomas that do arise often manifest advanced pathology (villous features, high-grade dysplasia) even at small sizes.53 Indeed, adenomas in patients with HNPCC often manifest MSI54 even in their earliest stages of formation. Because these adenomas tend to progress more rapidly to carcinoma,55,56 surveillance intervals for colonoscopy following removal of adenomas in HNPCC patients should be shortened (see later; see also Chapter 123).
Epidemiology and Etiology
Prevalence
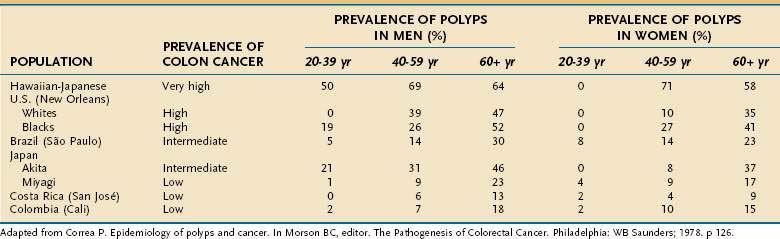
The prevalence of adenomatous polyps is affected by four major factors: the inherent risk for colon cancer in the population, age, sex, and family history of colorectal cancer. The frequency of colon adenomas varies widely among populations, but it tends to be higher in populations at greater risk for colon cancer (Table 122-5).10 One illustrative example is to compare the very high adenoma prevalence in Japanese living in Hawaii (a very high risk area for colon cancer) with the much lower adenoma prevalence in Japanese who still reside in Japan, an area of much lower risk. Even within Japan itself, adenoma prevalence correlates quite well with colon cancer prevalence in different prefectures of the country. Data from autopsy series provide an approximation of adenoma prevalence. In populations at low risk for colon cancer, adenoma prevalence rates are lower than 12% (see Table 122-5), whereas in most intermediate- and high-risk populations, adenomas are found in 30% to 40% of the population, and rates as high as 50% to 60% have been observed.7,57 One half to two thirds of people older than 65 years in high-risk areas can harbor colonic adenomas.7,57
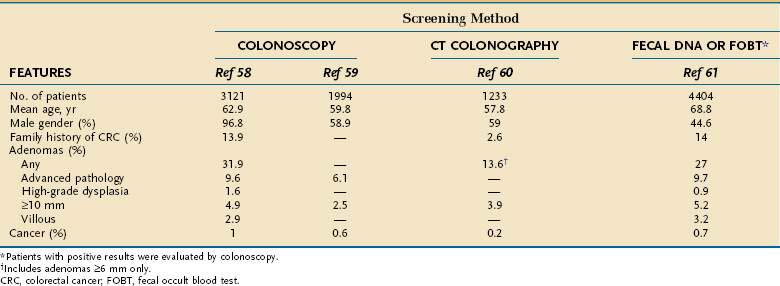
The true prevalence rate of adenomatous polyps within an asymptomatic population is only now being elucidated because, until recently, colonoscopy was not performed on healthy persons in the absence of gastrointestinal symptoms. Approximately 27% to 32% of asymptomatic average-risk persons older than 50 years undergoing screening colonoscopy will have an adenoma, and 6% to 10% will have an AAP (Table 122-6).58–61 By comparison, colonoscopic screening of asymptomatic persons between 40 and 49 years of age revealed prevalence rates of only 8.7% for tubular adenomas and 3.5% for AAP or cancer.62 Colonoscopic series indicate that men have a 1.5 relative risk of adenomas compared with age-matched women,62,63 thus confirming earlier observations in autopsy series.8,11 Men also have slightly higher rates of advanced adenomas than do women, with a relative risk of approximately 1.5.64 A large database study found a higher rate of polyps larger than 9 mm in African Americans undergoing screening colonoscopy compared with age-matched whites.65
The prevalence of adenomas is higher in older people, particularly those older than 60 years. In fact, age is the single most important independent determinant of adenoma prevalence7,11,12,57,62,63,66,67 in high-risk and low-risk regions of the world (see Table 122-5). Not only is advancing age associated with a higher prevalence rate of adenomas, but it also correlates with a greater likelihood for multiple polyps, adenomas with more severe degrees of dysplasia, and, in some studies, larger adenomas.
Adenoma prevalence also is higher in persons with a family history of colorectal cancer and adenomas,67,68 particularly if more than one relative is affected with colorectal neoplasia and if the affected relative is young.
Incidence
Estimating the incidence of new adenomas requires examining the colon at more than one point in time. Two types of endoscopic studies lend themselves to this analysis: surveillance studies following polypectomy (or following cancer resection) and interval examinations in persons who initially had a negative examination. Of course, for both types of studies, the small but measurable miss rate of adenomas can influence the rate of apparent incident adenomas (see “Detection,” later). For the purposes of this discussion, adenomas found in persons after polypectomy are considered recurrences (see “Postpolypectomy Management”), whereas those found in persons after an initial negative colonoscopy are considered incident adenomas.
The incidence of new adenomas varies from 24% to 41%.63 In one study, patients underwent colonoscopy twice on the same day to clear the colon of all potentially missed adenomas, and 38% were found to have new adenomas at colonoscopy two years later.69 Three-year follow-up sigmoidoscopy after an initial negative examination in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial found a 3.1% incidence of all adenomas and 0.8% incidence of advanced adenomas or cancer.70 A large surveillance study looked at findings on follow-up colonoscopy performed within 5.5 years of the index colonoscopy. Patients who had one or two tubular adenomas less than 10 mm were no more likely to have advanced neoplasia than patients with negative baseline colonoscopies. In average-risk, asymptomatic persons with no adenomas at baseline colonoscopy, repeat colonoscopy within five years detects an adenoma in approximately 16% to 27%71,72 and an AAP in approximately 1% to 2.4%.71–73
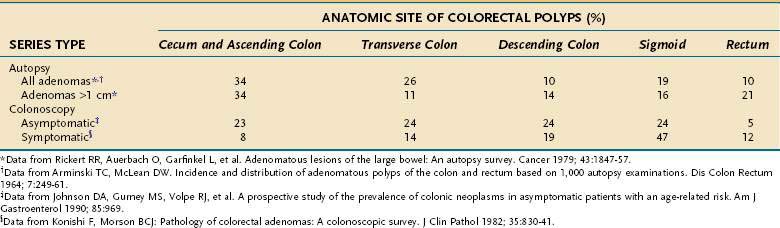
Anatomic Distribution
The distribution of adenomatous polyps within the colon differs, depending on the method of investigation (Table 122-7). In autopsy series in which the normal distribution is approximated in presumably asymptomatic subjects, adenomas are distributed uniformly throughout the colorectum; this even distribution has been confirmed in colonoscopic investigations of asymptomatic subjects.23,57 Large adenomas in autopsy series have a distal predominance, in the region where most colon cancers arise, thereby supporting the adenoma-carcinoma hypothesis. Likewise, adenomas detected in surgical and colonoscopic studies of symptomatic people also display a left-sided predominance, indicating that distal adenomas are more likely to come to clinical attention. In older persons, particularly those older than 60 years, distribution of adenomas demonstrates a shift toward more proximal colonic locations. This phenomenon, which is based on autopsy11,12 and on colonoscopic studies of symptomatic74 and asymptomatic22,58,59,66,75 subjects, has importance for choosing appropriate colon cancer screening approaches (see Chapter 123). Some data suggest that African Americans have a greater proportion of proximal adenomas compared with whites, especially in persons older than 60 years.65
Risk Factors for Susceptibility to Adenomas
Evidence is mounting to suggest that both heredity and environment contribute to susceptibility to colonic adenomas. Indeed, the interplay between genetic predisposition and environmental factors supports a hypothesis proposed by Hill many years ago concerning adenoma causation, which was based mainly on epidemiologic and histopathologic observations.76
Related posts:
 Surgical Peritonitis and Other Diseases of the Peritoneum, Mesentery, Omentum, and Diaphragm
Surgical Peritonitis and Other Diseases of the Peritoneum, Mesentery, Omentum, and Diaphragm
 Hepatitis Caused by Other Viruses
Hepatitis Caused by Other Viruses
 Hemochromatosis
Hemochromatosis
 Gastrointestinal and Hepatic Complications of Solid Organ and Hematopoietic Cell Transplantation
Gastrointestinal and Hepatic Complications of Solid Organ and Hematopoietic Cell Transplantation
 Nutritional Assessment and Management of the Malnourished Patient
Nutritional Assessment and Management of the Malnourished Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


