Chapter 49 Chronic Pancreatitis, Stones, and Strictures
 Video related to this chapter’s topics: Pancreatic Duct Stone Extraction
Video related to this chapter’s topics: Pancreatic Duct Stone Extraction
Introduction
Chronic pancreatitis is an inflammatory condition that results in permanent structural changes in the pancreas, which can lead to impairment of exocrine and endocrine function.1 This disorder contrasts with acute pancreatitis in that the latter is nonprogressive, and the gland returns to histologic and functional normalcy once the acute event subsides. Most diagnostic and therapeutic efforts in chronic pancreatitis are directed toward evaluation and management of symptoms, primarily abdominal pain and steatorrhea. Although interpretation of data on the role of endoscopic therapy for management of chronic pancreatitis remains difficult, this area is rapidly expanding and is of great interest and challenge to gastrointestinal endoscopists.
Epidemiology
The incidence of chronic pancreatitis is in the range of 3 to 10 per 100,000 population in many parts of the world.2 The crude incidence rate for chronic pancreatitis per 100,000 population in Germany is 6.4; in Czech Republic, 7.9; and in Japan, 27.9.3–5 The peak incidence for chronic pancreatitis in Germany is in the age group 45 to 54 years, which is 10 years older than the peak age group for acute pancreatitis suggesting that chronic pancreatitis develops during this time frame following first attacks of acute pancreatitis. In a prospective study that evaluated patients with alcoholic chronic pancreatitis, an annual incidence of 8.2 cases per year per 100,000 population and an overall prevalence of 27.4 cases per year per 100,000 population were noted.6 The incidence rates in retrospective European and North American studies range from 2 to 10 per 100,000 cases per year.7,8 Chronic pancreatitis is more common in male patients3,5,6; the male-to-female ratio in Japan is 3.5.5 Compared with whites, blacks are two to three times more likely to be hospitalized for chronic pancreatitis than for alcoholic cirrhosis.9 The explanation for this observation is unclear but could be related to racial differences in diet, type or quantity of alcohol consumption, smoking, or ability to detoxify substances harmful to the liver or pancreas. The absence of any screening programs and unresolved debate on the “gold standard” for diagnosis of chronic pancreatitis make epidemiologic studies in this area more difficult and explain the wide range of variations noted among studies.
Pathophysiology
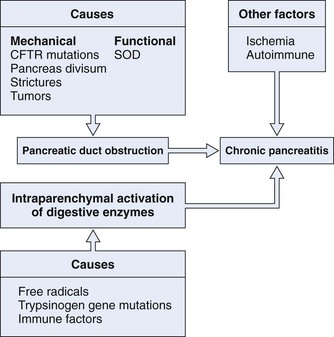
The pathogenesis of chronic pancreatitis seems to be multifactorial and is probably initiated by two distinct events (Fig. 49.1). The first event is a decrease in bicarbonate secretion that is due to either a mechanical or a functional ductal obstruction. Mechanical causes include strictures, sphincter of Oddi dysfunction, and tumors. Functional causes include mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene leading to impaired bicarbonate secretion. This impaired bicarbonate secretion has formed the basis for the secretin pancreatic function test. The second event involves intraparenchymal activation of digestive enzymes within the pancreatic gland. Ischemia, antioxidant stress, and sphincter of Oddi dysfunction are possible later events involved in perpetuating the disease process. This multifactorial model provides an explanation as to why no single therapy works in all patients with chronic pancreatitis.
Pancreatic Duct Obstruction
Proteinaceous plugs are one of the earliest findings noted in patients with chronic pancreatitis.10 It is theorized that increased glandular secretion of pancreatic proteins causes precipitation of proteinaceous plugs within the pancreatic ductal system. These plugs may act as a nidus for calcification that leads to stone formation. As ductal obstruction progresses, inflammatory changes and cell loss occur. The importance of these proteinaceous plugs in perpetuating changes within the pancreas is emphasized by studies that have shown relief of clinical symptoms after endoscopic removal of these plugs in patients with chronic pancreatitis.11,12 GP2 is a glycosyl phosphatidylinositol anchored protein that is cleaved from the zymogen granules and secreted into the pancreatic juice. This protein has been identified as a major component of intraductal plugs.13 Pancreatic acinar cells release another protein called lithostatine that prevents calcium carbonate precipitation and stone formation in pancreatic juice.14 Low levels of these proteins in patients with chronic pancreatitis may be another factor involved in stone formation.
Ischemia
Ischemia may be another important event in the pathogenesis of chronic pancreatitis. Animal models have shown that partial pancreatic duct ligation induces ductal hypertension and increased resistance to blood flow within the pancreas.15,16 Blood flow was found to be 40% of that observed in controls. Secretory stimulus reduced blood flow further as opposed to the normal increase. In patients with chronic pancreatitis, pancreatic interstitial pressure increases to a greater degree than in normal individuals owing to decreased glandular elasticity. The rapid relief of symptoms achieved by ductal decompression procedures suggests that ischemia plays a central role in the complex mechanisms involved in chronic pancreatitis.
Antioxidants
Nutritional depletion is frequently seen in patients with chronic pancreatitis. In particular, antioxidants such as selenium, vitamin C and E, and methionine are depleted.17,18 An imbalance between a decrease in antioxidants and an increased demand for them in pancreatic cells in chronic pancreatitis may lead to elevation in free radical formation, which is associated with lipid peroxidation and cellular impairment. Increased membrane lipid peroxidation, a marker of oxidative stress and free radical production, can also be seen in alcoholic chronic pancreatitis.19 It is postulated that alcohol causes a disproportionate increase in the secretion of trypsinogen leading to premature activation of digestive enzymes within the acinar or ductal cell systems.20
Autoimmunity
Chronic pancreatitis is also seen in association with autoimmune disorders such as Sjögren’s syndrome and primary biliary cirrhosis.21,22 Autoantibody to pancreatic antigens has been shown in patients with Sjögren’s syndrome and idiopathic chronic pancreatitis. Some cases of idiopathic chronic pancreatitis are associated with the expression of novel HLA-DR antigens on duct cells in combination with a localized T-cell inflammatory infiltrate, lending further credibility to an autoimmune pathogenesis.23
Interstitial Fibrosis
It is proposed that repeated episodes of acute pancreatitis initiate a sequence of perilobular fibrosis, duct distortion, and altered secretion and flow of pancreatic juice.24 Studies on the natural history of pancreatitis have shown that more frequent and more repeated attacks of acute pancreatitis lead to chronic changes as seen in the alcoholic type of chronic pancreatitis.25 The exact mechanisms involved in the pathophysiology of chronic pancreatitis are still elusive and unproven. Multiple exogenous factors may act in a genetically predisposed patient in an appropriate clinical setting, such as alcohol consumption, to trigger a cascade of events culminating in progressive destruction of pancreatic parenchyma and ensuing sequelae. Although the focus of therapies has been the inhibition of acinar cell secretion, further insights into the role of ductal bicarbonate secretion, ductal obstruction, and the relative contribution of ischemia and oxygen-derived free radicals in this process may provide new therapeutic avenues.
Etiology
Alcohol
Alcohol abuse accounts for 70% to 80% of cases of chronic pancreatitis (Table 49.1); the mechanism by which this occurs is unclear. The risk seems to be related to the duration and amount of alcohol consumed rather than the type of alcohol or the pattern of consumption.26 Intake of large amounts of alcohol (>50 g/day) has been shown to be associated with a shortened time to pancreatic calcification and survival.27 There is considerable variation in individual sensitivity to the toxicity of alcohol making it difficult to define a “safe” level of consumption. Only 5% to 10% of alcoholics develop chronic pancreatitis, suggesting that other unidentified factors may be important in the pathogenesis of the disease.28 Tobacco, although not important in the pathogenesis of alcoholic pancreatitis,29,30 has been implicated in the development of calcification in patients who already have chronic pancreatitis.31 A U.S.-based study showed an association between the presence of calcium-sensing receptor gene polymorphisms and chronic pancreatitis.32 The risk for developing chronic pancreatitis was significantly higher in patients with these gene polymorphisms who consumed moderate to heavy amounts of alcohol.
Table 49.1 Etiology of Chronic Pancreatitis
| Alcohol | 70% |
| Idiopathic | 10%–30% |
| Other | 10%–15% |
| Pancreatic duct obstruction (trauma, divisum, tumor, fibrosis) | |
| Hereditary (CFTR gene mutation, trypsinogen gene mutation) | |
| Hyperlipidemia | |
| Tropical |
CFTR, cystic fibrosis transmembrane conductance regulator.
Hereditary Pancreatitis
Hereditary pancreatitis is characterized by a young age at onset and prominent pancreatic calcifications. It is transmitted as an autosomal dominant trait, and nearly 80% of patients with the inherited defect develop chronic pancreatitis.33 Most affected individuals develop symptoms before age 20. In some kindreds, hereditary chronic pancreatitis has been mapped to the long arm of chromosome 7 (7q35), where a cluster of trypsinogen genes is located.34,35 Several mutations associated with chronic pancreatitis have been identified in this region. Although the exact consequences of these mutations on trypsin activity are unclear, they are known to interfere with trypsin inactivation or to enhance its activation, permitting autodigestion of the pancreas.36,37 Although mutations in the trypsinogen gene are specific for hereditary pancreatitis, not all affected family members develop chronic pancreatitis. The relationship between mutations of other genes associated with chronic pancreatitis, such as the CFTR and the trypsinogen genes, needs further elucidation.
Mutations of the Cystic Fibrosis Gene
Cystic fibrosis is due to mutations in the CFTR gene. Most patients with cystic fibrosis develop progressive pancreatic damage as a result of defective ductular and acinar pancreatic secretion.38 In some series, mutations in the CFTR gene have been identified in 13% to 37% of patients with idiopathic chronic pancreatitis who have no clinical evidence of cystic fibrosis.39,40 This percentage range could be an underestimation because currently available genetic screening tests identify only 18 to 23 of the most severe CFTR mutations that cause classic, childhood cystic fibrosis.
Tropical Pancreatitis
Tropical pancreatitis is a condition of unknown etiology that is seen commonly in younger individuals in south India and other parts of the tropics, where it is the most common cause of chronic pancreatitis. The pathology is characterized by large intraductal calculi, marked dilation of the pancreatic ducts, atrophy, and fibrosis. Clinically, most patients experience abdominal pain, diabetes mellitus, and fat malabsorption. The etiology of tropical pancreatitis is unknown. The cassava fruit had been implicated as an etiologic factor in this disorder, although it is no longer thought to be related.41 Mutations in the serine protease inhibitor SPINK1 have been identified in some patients.42,43
Ductal Obstruction
Obstruction of the pancreatic duct from any cause can lead to chronic pancreatitis. The histologic abnormalities that are induced may persist after relief of the obstruction. Sphincter of Oddi dysfunction seems to be associated with chronic pancreatitis. In one study of patients with chronic pancreatitis undergoing sphincter of Oddi manometry, more than 60% had sphincter of Oddi dysfunction.44
Pancreas divisum may cause chronic pancreatitis by producing a relative obstruction to flow of pancreatic juice at the minor papilla. It is estimated that less than 5% of patients with pancreas divisum develop pancreatic symptoms. The low frequency of symptoms has created controversy as to whether pancreas divisum and its associated small minor papilla orifice are ever a cause of obstructive pancreatitis. The arguments against an association are based on two major observations. First, some studies have found that the incidence of pancreas divisum is the same among patients with and without pancreatitis.45 Second, symptoms occur infrequently in patients with this anomaly. We believe that there is a group of patients with pancreas divisum who are subject to recurrent bouts of seemingly idiopathic pancreatitis. In these patients, the minor papilla orifice is so small that excessively high intrapancreatic dorsal ductal pressure occurs during active secretion, which may result in inadequate drainage, ductal distention, pain, and, in some cases, pancreatitis. To support this view, greater than 60% of patients with pancreas divisum and otherwise unexplained abdominal pain had relief of pain after surgical sphincteroplasty suggesting that obstruction to flow of secretion was the proximate cause of symptoms in these patients.46
Idiopathic Chronic Pancreatitis
An etiology for pancreatitis cannot be determined in 10% to 30% of patients with chronic pancreatitis despite extensive investigations. Concealed alcohol ingestion, hypersensitivity to small amounts of alcohol, unreported pancreatic trauma, and mutations in the CFTR and the trypsinogen genes may be contributing factors in at least a small proportion of patients with idiopathic chronic pancreatitis.47,48 Although in the past patients with idiopathic chronic pancreatitis were considered as a single group, data from the Mayo Clinic have defined an early and late onset form of idiopathic chronic pancreatitis.49 Age distribution at onset of symptoms showed a bimodal distribution of patients with early and late onset idiopathic chronic pancreatitis with a median age of 19.2 years for early onset and 56.2 years for late onset. No gender differences were observed among patients in either group. Pain was the predominant symptom in 96% of patients with early onset idiopathic pancreatitis but was present in only 54% of late onset idiopathic pancreatitis. Regardless of whether patients had early or late onset idiopathic pancreatitis, pain was the presenting symptom, and endocrine and exocrine insufficiency with pancreatic calcification was seen in both forms of the disease.
Clinical Features
Abdominal Pain
The mechanism for abdominal pain is poorly understood. Causes are perhaps multifactorial and include inflammation, duct obstruction, high pancreatic tissue pressure, fibrotic encasement of sensory nerves, and neuropathy characterized by both increased numbers and sizes of intrapancreatic sensory nerves and by inflammatory injury to the nerve sheaths allowing exposure of the neural elements to toxic substances.50,51 Pain is not in the spectrum of clinical symptoms in nearly one-fourth of patients with chronic pancreatitis.52 The view that chronic pain subsides in a substantial number of patients as the disease progresses to the point of organ failure53 has been widely accepted, but that process may take an unpredictable number of years or may never occur. Some studies suggest that the likelihood of spontaneous pain relief is low.54 In a study that evaluated the natural history of pain in chronic pancreatitis, pain decreased or disappeared in 67%, 64%, and 77% of early onset idiopathic, late onset idiopathic, and alcoholic pancreatitis over a median time of 25 years, 13 years, and 14 years.49
Pancreatic Insufficiency
Patients with severe pancreatic exocrine dysfunction cannot properly digest complex foods or absorb digestive breakdown products. Nevertheless, clinically significant protein and fat deficiencies do not occur until more than 90% of pancreatic function is lost.55 In a large natural history study, the median time for development of pancreatic insufficiency was 13.1 years in patients with alcoholic chronic pancreatitis, 16.1 years in patients with late onset idiopathic chronic pancreatitis, and 26.3 years in patients with early onset idiopathic chronic pancreatitis.48 Steatorrhea usually occurs before protein deficiencies because lipolytic activity decreases more quickly than proteolysis.56,57 Glucose intolerance occurs frequently in chronic pancreatitis, but overt diabetes mellitus usually occurs late in the course of disease. Patients with chronic calcific disease, particularly patients who develop early calcifications, may develop diabetes more frequently than patients with chronic noncalcific disease.58,59 Nearly 40% to 70% of patients with chronic pancreatitis develop diabetes on prolonged follow-up. In one study, the median time to develop diabetes was 19.8 years, 11.9 years, and 26.3 years in patients with alcoholic, late onset idiopathic, and early onset idiopathic chronic pancreatitis.49 In chronic pancreatitis, both insulin-producing beta cells and glucagon-producing alpha cells are destroyed. When exogenously administered insulin leads to hypoglycemia, the deficiency in glandular glucagon storage fails to correct the serum glucose levels back to normal leading to prolonged and severe hypoglycemia. The nature of diabetes in this patient population is brittle, and management is more complicated than that of patients with type 1 diabetes.
Pathology
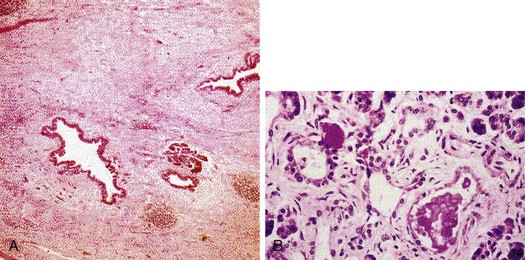
In early stages of chronic pancreatitis, glandular damage is patchy and uneven (Fig. 49.2). Areas of irregularly distributed fibrosis, reduced number and size of acini with relative sparing of the islets of Langerhans, and variable degrees of obstruction of pancreatic ducts of all sizes are seen.60 A chronic inflammatory infiltrate around lobules and ducts is usually present. The interlobular and intralobular ducts are dilated and contain protein plugs in their lumens. The ductal epithelium may be atrophied or hyperplastic or show squamous metaplasia, and ductal concretions may be evident. Remaining islets become embedded in sclerosed tissue or severely damaged lobules before they too disappear. Grossly, the gland is hard, sometimes with extremely dilated ducts and grossly visible calcified concretions. Pseudocyst formation is common.
Differential Diagnosis
The International Pancreatitis Study Group observed a standardized incidence ratio for pancreatic cancer of 26.3 among patients with chronic pancreatitis compared with an expected ratio of 2.13 that was calculated from country-specific incidence data and adjusted for age and sex.61 Similar to chronic pancreatitis, patients with pancreatic cancer can present with abdominal pain, weight loss, and jaundice. Findings suggestive of possible pancreatic cancer in a patient thought or known to have chronic pancreatitis include older age, absence of a history of alcohol use, weight loss, a protracted flare of symptoms, and the onset of significant constitutional symptoms. The physician should maintain a high index of suspicion for pancreatic cancer, particularly in any elderly patient presenting with a new-onset pancreatitis when common causes such as alcohol and gallstones have been excluded. Tumor markers such as CA 19.9 (for colorectal and pancreatic carcinomas) and carcinoembryonic antigen (CEA) are helpful if elevated, but normal values do not rule out pancreatic cancer. Computed tomography (CT) or endoscopic ultrasound (EUS)–guided biopsy may be required to establish the diagnosis in some patients.
Diagnosis
Tests for chronic pancreatitis can be classified into tests that evaluate the structure of the gland (parenchyma, ductal anatomy, or both) or its exocrine function (Table 49.2). The tests most widely used clinically are tests that assess structure. The clinical manifestations of pancreatic insufficiency are usually a late event in the course of chronic pancreatitis when more than 90% of the glandular tissue is not functioning either because of glandular dysfunction or because of fibrotic tissue replacement or proximal pancreatic duct obstruction. The most sensitive and accurate among pancreatic function tests is the secretin stimulation test. However, this test is invasive, its methodology is very time-consuming and demanding, and its diagnostic accuracy is not superior to endoscopic retrograde cholangiopancreatography (ERCP).62,63 Noninvasive pancreatic function tests yield sufficient diagnostic accuracy only in the advanced stages of the disease, and their sensitivity for detection of early or moderate chronic pancreatitis is low.64 Tests that evaluate pancreatic structure, although limited by sensitivity, are advantageous in that they are more widely available and are better standardized for clinical use.
Table 49.2 Diagnostic Tests for Chronic Pancreatitis
| Structural Tests | Functional Tests | |
|---|---|---|
| Indirect | Direct | |
| X-ray | Serum enzymes (trypsinogen) | Secretin stimulation test |
| Ultrasound | Fecal tests (fat, elastase, chymoptrysin) | |
| CT | Urine tests (bentiromide, pancreolauryl) | |
| MRCP | ||
| ERCP | ||
| EUS | ||
CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound; MRCP, magnetic resonance cholangiopancreatography.
Tests of Pancreatic Function
Invasive or Direct Pancreatic Function Tests (Secretin Stimulation Test)
Some studies have shown the secretin stimulation test to be slightly more sensitive than ERCP for the diagnosis of chronic pancreatitis, but the evaluation of all tests in the diagnosis of chronic pancreatitis is suspect because of the lack of a “gold standard.” Sensitivity ranges from 74% to 97%, and specificity ranges from 80% to 90%.63,65–69 The percentage of patients with an abnormal stimulation test and a normal pancreatogram ranges from 3% to 20%.66–69 When such patients were followed, two studies found that 90% of patients developed chronic pancreatitis.69,70 Conversely, these studies also identified a small group of patients (<10% on average) with a normal hormonal stimulation test but an abnormal pancreatogram. On long-term follow-up, chronic pancreatitis developed in 0% to 26% of patients.69,70 When the results of pancreatic function tests were compared with pancreatic histology, the overall sensitivity, specificity, and accuracy were 67%, 90%, and 81%.71 Limitations of this test are that it is not well accepted by patients, it is time-consuming and expensive, and it requires specialized equipment and methodology. The test has not been well standardized, and a consensus on the normal ranges for the test results is yet to be reached. The test is available in very few specialized pancreatic centers around the world.
Noninvasive or Indirect Pancreatic Function Tests
Serum Enzymes
Because chronic pancreatitis is a patchy, focal disease with significant parenchymal fibrosis, pancreatic serum enzyme levels (amylase and lipase) are not or only minimally elevated. Very low levels of serum trypsinogen (<20 ng/mL) are reasonably specific for chronic pancreatitis, but levels as low as this are seen only in very advanced stages of the disease where there is accompanying steatorrhea.55 In clinical practice, serum enzyme levels are helpful to identify an acute attack of chronic pancreatitis or for monitoring the disease evolution with abnormally low concentration once steatorrhea occurs.
Fecal Tests
Steatorrhea can be diagnosed qualitatively by Sudan staining of feces or quantitatively by determination of fecal fat excretion over 72 hours while the patient is consuming a 100 g/day fat diet for at least 3 days before the test. Excretion of more than 7 g of fat per day is diagnostic of malabsorption, although patients with steatorrhea often have values greater than 20 g/day. On qualitative analysis, more than six globules per high-power field is considered to be positive, but the patient must be ingesting adequate fat to allow measurable steatorrhea. In a landmark study on exocrine insufficiency, steatorrhea did not occur until more than 90% of the pancreas or more than 85% of pancreatic lipase had been destroyed.55 Stool fat analysis has limited sensitivity in chronic pancreatitis because patients with mild and moderate and often severe chronic pancreatitis in the absence of steatorrhea would not be detected by this technique. A novel method, near-infrared reflectance analysis (NIRA), may become the procedure of choice for evaluating fat malabsorption.72–74 NIRA is equally accurate but less time-consuming than a 72-hour fecal fat collection and allows for simultaneous measurement of fecal fat, nitrogen, and carbohydrates in a single sample. NIRA is being increasingly used in Europe and is available in some centers in the United States.
The low diagnostic value of fat malabsorption in chronic pancreatitis led to the discovery of individual pancreatic enzymes in stool specimen that have increased diagnostic sensitivity. Measurement of fecal chymotrypsin is abnormal in most patients with chronic pancreatitis and steatorrhea.65 Since inception of fecal chymotrypsin measurement into clinical use, its utility has been clearly established only in advanced chronic pancreatitis with exocrine insufficiency. This assay is unavailable in the United States at the present time. More recently, an assay to measure human pancreatic elastase in feces has been developed. The assay detects exclusively human elastase, and so no interference occurs with simultaneous therapeutic pancreatic enzyme supplementation. The diagnostic sensitivity and specificity of the fecal elastase test are superior to the fecal chymotrypsin test, although both tests are most accurate in advanced chronic pancreatitis.75 The fecal elastase test may be falsely abnormal in other diseases causing steatorrhea, such as short bowel syndrome or small bowel bacterial overgrowth syndrome. This test is available but not widely used in the United States.
Urine Tests
The principle of urine tests is based on the administration of a complex substrate, which is hydrolyzed by a specific pancreatic enzyme with the release of a pancreatic marker substance. This marker is absorbed from the gut and detected and quantitated either in urine or in serum. The bentiromide (N-benzoyl-l-tyrosyl-p-aminobenzoic acid [NBT-PABA]) test measures the presence of pancreatic chymotrypsin within the gut lumen, and the pancreolauryl test measures the presence of pancreatic arylesterases within the gut lumen. Both tests are accurate in advanced chronic pancreatitis, with sensitivities of 80% to 100%.65 Limitations of these tests lie in the fact that both tests require anatomic and functional integrity of the digestive systems. Although these tests have reasonable accuracy, they are both unavailable for clinical use in the United States at the present time.
Tests of Pancreatic Structure
Plain Abdominal Radiography
Calcifications within the pancreas are present on plain films in about one-third of patients with chronic pancreatitis (Fig. 49.3). Calcifications occur late in the natural history of chronic pancreatitis and may take 5 to 25 years to develop.49,53 Both anteroposterior and oblique views should be employed because small flecks of calcium can be lost in the spine if oblique views are not obtained. The finding of calcification is pathognomonic of chronic pancreatitis, but the sensitivity of this test is very low.
Abdominal Ultrasound
Ultrasound was the first technique that allowed complete imaging of the pancreas. Several morphologic characteristics of chronic pancreatitis are detectable by ultrasound, including irregular contours in the margin of the gland, dilation and irregularity of the main pancreatic duct, heterogeneity of the gland parenchyma, cysts within or adjacent to the pancreas, and the presence of calcifications.76 The sensitivity and specificity of ultrasound for the diagnosis of chronic pancreatitis are 60% to 70% and 80% to 90%.77 However, the detail to which the pancreas can be interrogated depends on the body habitus of the patient, the presence or absence of overlying bowel gas, and the experience and expertise of the sonographer.
Computed Tomography
The sensitivity and specificity of CT for the diagnosis of chronic pancreatitis are 75% to 90% and 85%.65 The main advantage of CT is that it can be standardized and in virtually all cases can visualize the pancreas in its entirety. CT scan is the most sensitive test for detecting calcification, is accurate in detecting main pancreatic duct dilation, and can detect an irregular contour of the gland (Fig. 49.4).65,78,79 These features are characteristics of advanced chronic pancreatitis, and CT is quite good at detecting these changes. However, CT is poor at detecting subtle abnormalities in pancreatic parenchyma or changes in side branches of the pancreatic duct, which are commonly seen in milder forms of the disease. CT has good specificity but lacks sensitivity for diagnosis of chronic pancreatitis. The newer spiral CT scanners would be likely to produce better sensitivity.

Magnetic Resonance Cholangiopancreatography
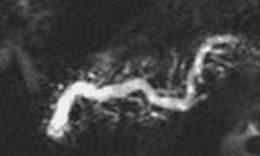
Several small studies have reported on the utility of magnetic resonance cholangiopancreatography (MRCP) in assessing pancreatic duct morphology.80,81 MRCP agrees with ERCP in 70% to 80% of findings, with higher rates of agreement in studies using the most advanced image analysis techniques (Fig. 49.5). In studies that compared MRCP findings with ERCP, MRCP visualized the main pancreatic duct in the head, body, and tail in 79%, 64%, and 53% of cases.82 Correlation with ERCP with respect to main pancreatic duct dilation, narrowing, and filling defects was 83% to 92%, 70% to 92%, and 92% to 100%. The major disadvantage of MRCP compared with conventional cholangiography is a lower spatial resolution, such that MRCP continues to be partially limited in the assessment of fine detail, such as subtle side branch changes of chronic pancreatitis. Improvements in magnetic resonance (MR) imaging analysis are expected to continue to improve the image quality of MRCP, and image quality could approach ERCP in accuracy in the future.
Endoscopic Retrograde Cholangiopancreatography
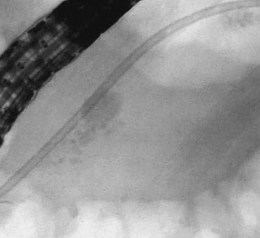
ERCP is the most widely used structural test for chronic pancreatitis (Fig. 49.6). In 1984, the Pancreatic Society of Great Britain and Ireland reached a consensus on ductographic definitions for chronic pancreatitis, known as “the Cambridge criteria,” which have become the most widely accepted criteria for interpreting pancreatography.83 The criteria are based on abnormalities seen in the main pancreatic duct and side branches (Table 49.3). In most studies, the sensitivity of ERCP is 70% to 90%, and specificity is 80% to 100%.63,65–69 ERCP is highly sensitive and specific in patients with advanced structural disease; less dramatic pancreatographic changes are less definitive.84,85 The ductographic abnormalities of chronic pancreatitis are not specific; age-related changes, morphologic changes such as in pancreatic cancer or recovery phase of acute pancreatitis, and injury induced by stent treatment can mimic chronic pancreatitis.

Table 49.3 Cambridge Grading of Chronic Pancreatitis by Endoscopic Retrograde Pancreatography
| Grade | Main Pancreatic Duct | Side Branches |
|---|---|---|
| Normal | Normal | Normal |
| Equivocal | Normal | <3 abnormal |
| Mild | Normal | >3 abnormal |
| Moderate | Abnormal | >3 abnormal |
| Severe | Abnormal, with at least one of the following | >3 abnormal |
| Large cavity (>10 mm) | ||
| Duct obstruction | ||
| Intraductal filling defects | ||
| Severe dilation or irregularity |
Adapted from Axon AT, Classen M, Cotton PB, et al: Pancreatography in chronic pancreatitis: International definitions. Gut 25:1107, 1984.
Chronic pancreatitis can involve the pancreatic parenchyma per se and completely spare the radiographically visible portions of the pancreatic ductal system leading to false-negative studies.86,87 Also, significant interobserver and intraobserver variability is noted in the interpretation of pancreatography.88 Much of this variability is related to interpretation of mild pancreatographic changes rather than to severe abnormalities. There are several limitations with ERCP as a diagnostic test for chronic pancreatitis. Reliable interpretation of ERCP depends on adequate filling of the pancreatic duct with dye such that the secondary branches are well visualized. However, inadequate opacification of ducts, especially the secondary ducts, occurs in at least 30% of cases.84 The procedure is invasive and is associated with a 3% to 7% chance of causing acute pancreatitis.89 This risk is low in patients with advanced disease and high in patients with mild disease, particularly patients with underlying sphincter of Oddi dysfunction.90
Endoscopic Ultrasound
Numerous EUS criteria for pancreatic disease have been described (Fig. 49.7). Lees and colleagues91,92 first described EUS findings in patients with clinical and radiologic evidence of chronic pancreatitis and characterized EUS criteria that distinguish normal from abnormal pancreas. Wiersema and associates93 refined their definitions and found that abnormal EUS changes occurred frequently in patients with abnormal endoscopic pancreatograms and were absent in healthy volunteers. Criteria for chronic pancreatitis that are specific to EUS can be divided into two groups (Table 49.4): parenchymal and ductal. Parenchymal criteria include inhomogeneity, hyperechoic foci, hyperechoic strands, cysts, and lobularity. Ductal criteria specific to EUS include obvious to more subtle ductal dilation (≥3 mm in the head, ≥2 mm in the body, ≥1 mm in the tail), hyperechoic main duct margins, irregular main duct margins, and visible side branches.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


