Fig. 15.1
The internal magnetic grasper (IMANLAP Ltd) can be (a) disposable or (b) reusable and is composed of a spring-loaded alligator clamp linked to an (c) 11.83-mm neodynium magnet. (d) The jaws of the alligator clamp (previously opened with the Thomas grasper™) are fastened tightly to the gallbladder’s fundus (arrow). The gallbladder is tractioned cephalad and retracted over the liver edge towards the patient’s right shoulder

Fig. 15.2
(a) The external magnet (IMANLAP Ltd), coupled to its articulating self-retaining arm, is placed over the patient’s abdominal wall. The laparoscope allows the surgeon to operate (take note of the 5-mm instrument inserted through the working channel) and drive the camera simultaneously (remember the camera headlight is coupled to a different and independent line). Visualization at the point of dissection can also be fixed this way (observe the red light below the external magnet) without the need for cumbersome roticulating instruments. (b) New version of the articulating self-retaining arm (arrowhead), which can be easily manipulated with one hand. It is more flexible and articulated
15.2 Instruments and Devices
magnet-assisted laparoscopic surgery requires two sets of instruments and devices.
The first one comprises those specifically designed for magnet-assisted laparoscopic surgery as the Thomas grasper™ (IMANLAP Ltd, Buenos Aires, Argentina), the internal magnetic grasper, the external magnet, the Dominguez articulating self-retaining arm, and the Williams grasper™ (IMANLAP Ltd, Buenos Aires, Argentina) (Table 15.1).
Table 15.1
Special instruments and devices for MALS (IMANLAP, Buenos Aires, Argentina)
Instrument | Brand | Description | Image |
|---|---|---|---|
Internal dominguez magentic grasper internal magnetic grasper | IMANLAP Ltd, Buenos Aires, Argentina | It is a spring-loaded alligator clamp linked to an 11.83-mm neodynium magnet (5,000 Gauss or 0.5 Tesla) coated with steel. The newest versions are additionally coated with biocompatible plastic |  |
External dominguez magnetic device external magnet | IMANLAP Ltd, Buenos Aires, Argentina | Of major size and potency. It can be used solely or, as in the image, fixed to the Dominguez articulating self-retaining arm |  |
Thomas grasper™ | IMANLAP Ltd, Buenos Aires, Argentina | Size: 5-mm × 50-cm. Made of austenitic surgical steel, which is unaffected by magnetic fields. It has two converging indented arms to handle, open, close and remove the internal magnetic grasper by its alligator clip. It allows its easy position and reposition within the body cavity |  |
Williams grasper™ | IMANLAP Ltd, Buenos Aires, Argentina | Size: 5-mm × 50-cm. Curved, non-magnetic, roticulating and rigid grasper |  |
The internal magnetic grasper (IMANLAP Ltd) can be reusable—environmentally friendly—or disposable (Fig. 15.1). By covering the intracorporeal magnet with biocompatible plastic, attractions between the instruments and the magnet are impeded. Moreover this material prevents the alligator clamp from transmitting electricity to the abdominal wall and enables the use of monopolar hook even in those cases in which the electrocautery device is leaning on the alligator clamp. This new version of the internal magnetic grasper ensures its sterilization with ethylene dioxide and is far more practical as there is no need to disassemble it for cleansing.
With the aim of achieving an effective surgical manipulation of the target organ, flexible control of its application point is essential. Fixation of the internal magnetic grasper (IMANLAP Ltd) was consequently improved by linking the alligator clamp to the magnet via a flexible connector. This results in softer retraction movements as the distance between the barycenter of the magnet and the application point is reduced.
The Thomas grasper™ (IMANLAP Ltd) handles the jaws of the alligator clamp intracorporeally. It was specially designed to be unaffected by electromagnetic fields and with the necessary strength to open and close the alligator clamp. The force needed for these maneuvers is substantially greater than that required for any other routine endosurgical grasping action, what explains the reason why the internal magnetic grasper (IMANLAP Ltd) is held tightly at the application site and rarely becomes loose, being a safe and effective retraction tool. If by chance, the internal magnetic grasper is released, it can be rapid and easily managed with the Thomas grasper™ and attached where it corresponds.
The external magnet (IMANLAP Ltd) frees surgical assistants for other tasks and can enable the main surgeon to operate alone whenever coupled to the Dominguez articulating self-retaining arm fixed to the operating table. Since the external magnet can be easily engaged and disengaged from the arm, it is possible to use it manually when dynamic magnetic retraction is needed. However, when static magnetic retraction is required, the external magnet can always be re-engaged to the arm without difficulty (Fig. 15.2).
The second set comprises already existing instruments and devices as a single 12-mm trocar (any brand is suitable) to accommodate the 11.83-mm internal magnetic grasper (IMANLAP Ltd) or the SILS™ port (Covidien, New Haven, CT, USA) for operations requiring more extensive dissection or intraabdominal suturing. We recommend the use of a 10-mm, 27-cm, 0° laparoscope, with a 6-mm working channel (Karl Storz-Endoskope, Tuttlingen, Germany) because it allows surgeons to operate and drive the camera simultaneously (the camera headlight is coupled to a different and independent line) (Fig. 15.3). Commercially available 42-cm, 5-mm instruments (irrigation/aspiration devices, dissectors, graspers, scissors, forceps, harmonic scalpels, staplers, needle holders, etc), can be perfectly accommodated. The Thomas grasper™ (IMANLAP Ltd) and the 5-mm Hem-o-Lok clip applier (Weck Teleflex, Research Triangle Park, NC, USA) have been lengthened up to 45-cm, to enhance reach and to allow extra maneurability within the body cavity (Fig. 15.4). Regular transumbilical instruments with exaggerated curves or roticulating tips are impractical for magnet-assisted laparoscopic surgery because they transmit little torque and their movements are counteractive. We therefore prefer to use a 5-mm, gently curved non-roticulating grasper (Karl Storz-Endoskope).
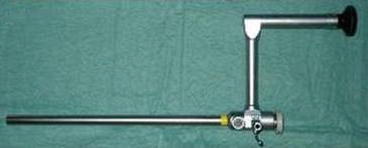
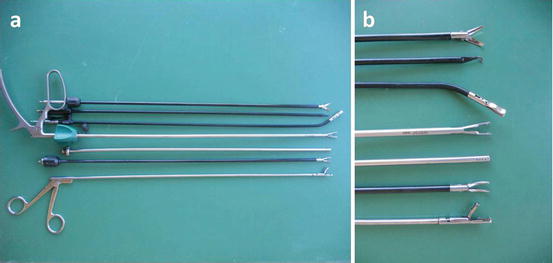
Fig. 15.3
10-mm, 27-cm, 0° laparoscope with a 6-mm working channel
Fig. 15.4
(a) Instruments and devices required to perform a transumbilical cholecystectomy with magnetic retraction. (b) A closer view to their tips. From left to right: Thomas grasper™ (IMANLAP Ltd), dissector, irrigation/aspiration device, Hem-o-Lok clip applier (Weck Teleflex), gently curved non-roticulating grasper, monopolar hook, scissor
15.3 Contraindications
The absolute constrainments are pregnancy and pacemaker patients.
The relative constrainments are:
Size of the patient: in those patients weighing <10 kg magnet-assisted laparoscopic surgery is unrecommended, as the internal magnetic grasper (IMANLAP Ltd) diameter is 11.83-mm, what means that at least a 12-mm trocar is needed. This trocar size can be too large for small patients as neonates or nursing babies. Moreover, the small size of the body cavity difficults a safe and effective movement of instruments and magnetic devices.
Thickness of the abdominal wall: for patients with a BMI >40 kg/m2, magnet-assisted laparoscopic surgery is not suggested as the thickened abdominal wall provokes a loss of tractive and/or repelling force of the magnet. However in patients undergoing bariatric surgery they can be safely used with a larger and more powerful external magnet (IMANLAP Ltd).
Adhesions, distance from the abdominal wall and weight of the tractive organ: can reduce the tractive force of the magnetic devices, though it is not necessarily a contraindication to magnet-assisted laparoscopic surgery.
15.4 Technique
Transumbilical Cholecystectomy with Magnetic Retraction, or in other words, magnet-assisted laparoscopic surgery of the gallbladder is founded on reproducing the classic laparoscopic cholecystectomy, with an optimum vision and exposition of the triangle of Calot. Before describing the technique, it must be pointed out that the technique can also be used as a complement in classic laparoscopic cholecystectomy since it clearly does not replace videosurgery but adds a surgical variant to the so called reduced port surgeries [11]. Additionally it makes possible the retraction of key structures without the need for needles, sutures and retractors permitting minimization of the number of access ports, incisions, and eventually staff.
General anesthesia is used in the same fashion as for a laparoscopic cholecystectomy. The patient’s umbilicus is infiltrated with local anaesthesia (bupivacaine) to facilitate an equilibrated analgesia. A single 1.5-cm umbilical incision for a 12-mm port is performed. Even though in the beginning, we used to create the 12/14-mm Hg pneumoperitoneum using a Veress needle, we nowadays prefer the Hasson’s technique, which is safe and recommendable since many years ago, and because it is the best alternative in those occasions in which a good exposition of the umbilical aponeurosis is indispensable for the extraction of surgical specimens.
15.5 TCMR with One Trocar and Assisted by Two internal magnetic grasper (IMANLAP Ltd)
The patient is placed in a reverse Trendenlenburg’s position slightly rotated to the left. Initially the surgeon would stand up between the legs with the assistant aside and the scrub nurse opposite to the assistant (French position). Nowadays we use the American position with the monitor placed at the head of the operating table (Fig. 15.5).

Fig. 15.5
Patient placed in the anti-Trendelenburg position and slightly rotated towards the left. The monitor (not seen in the picture) is placed at the head of the operating table. Transumbilical cholecystectomy with magnetic retraction permits operating on patients through one single incision, with one trocar and only one surgeon. Patients can therefore be operated on with less complications (as postoperative pain and wound infection), superlative cosmesis (scarless surgery) and inferior costs in comparison to other laparoscopic and transumbilical approaches
The approach is transumbilical in all patients. The umbilical stem is never removed to accomplish an excellent cosmetic result. The laparoscope is introduced through the 12-mm trocar. Once the first internal magnetic grasper (IMANLAP Ltd) is progressed into the abdominal cavity, it is manipulated under direct vision with the Thomas grasper™ (IMANLAP Ltd). The latter enables the surgeon to maneuver the alligator clamp (onward, from behind, laterally and from its tip) to further orient it towards the gallbladder whereas the magnet faces the parietal peritoneum.
The external magnet (IMANLAP Ltd) attached to the articulating self-retaining arm, is drawn near the patient’s skin to generate a magnetic field across the abdominal wall that allows the mobilization of the internal magnetic grasper (IMANLAP Ltd) in all directions to suit the surgeon’s need. The jaws of the alligator clamp are opened with the Thomas grasper™ (IMANLAP Ltd) and fastened tightly to the gallbladder’s fundus or Hartmann’s pouch. By moving the external magnet in the direction of the axilla, the liver is lifted cephalad exposing the gallbladder, which is retracted over the liver edge toward the patient’s right shoulder (Fig. 15.6). By repositioning the external magnet on the abdominal wall, the intraabdominal magnet moves to provide further traction. Because the magnet is not fixed at any level, it can freely cruise around the peritoneal cavity, extending the surgeon’s reach without the need for additional ports. Next, the laparoscope is removed and another internal magnetic grasper is inserted in the same way as the first one. This 2° internal magnetic grasper is placed in the infundibulum and managed by another external magnet to expose the triangle of Calot for its dissection (Fig. 15.7a) at first and for the cholecystectomy next (Fig. 15.7b, c).
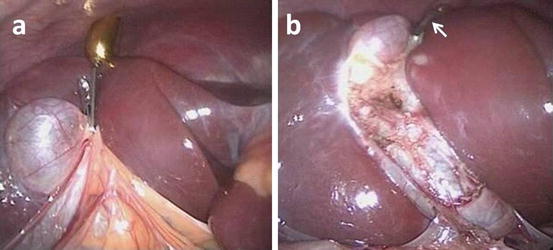
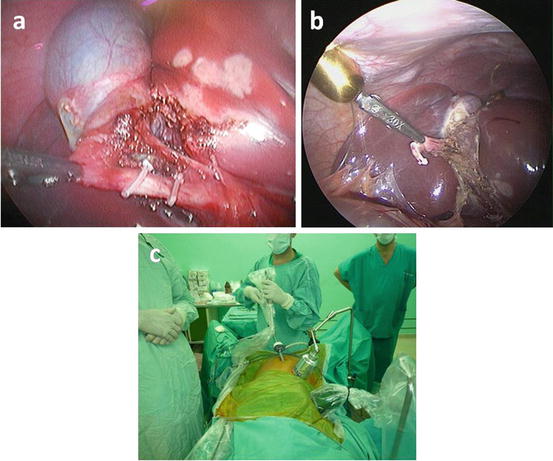
Fig. 15.6
The 1° internal magnetic grasper (IMANLAP Ltd) is used (a) to grasp the gallbladder and once the adhesions are released (b) to retract its fundus over the liver edge (arrow)
Fig. 15.7
The 2° internal magnetic grasper (IMANLAP Ltd) is placed in the infundibulum to expose the triangle of Calot as in (a). The cystic duct is sealed with proximal Hem-o-lok clips (Weck Teleflex). The gallbladder is dissected with an insulated hook. In (b) the 2° internal magnetic grasper is placed in the infundibulum and managed by a 2° external magnet (c) to complete the cholecystectomy
Once the surgical field is exposed, each 5-mm diameter instrument can be passed through the laparoscope’s 6-mm working channel for the cystic duct and vessels dissection, ligation and section, the cholangiography (whenever necessary), and the gallbladder dissection in the usual way that traditional laparoscopic cholecystectomy is performed. The cystic duct is sealed with a proximal medium sized Hem-o-lok polymer clip using the Hem-o-lock ligation applier, size M-L (Weck Teleflex) (Fig. 15.7a). The gallbladder is dissected at its base using an insulated hook. Finally, both internal magnetic grasper (IMANLAP Ltd) are released using the Thomas grasper™ (IMANLAP Ltd) and removed through the umbilical 12-mm trocar. The gallbladder is withdrawn under direct vision.
15.6 Transumbilical Cholecystectomy with Magnetic Retraction with One internal magnetic grasper: The Hybrid Method
The inconvenient of working with two internal magnetic grasper (IMANLAP Ltd) within the body cavity is the possibility of interactions produced between them. Despite this is infrequent when handled by experts, it can easily be solved by adding a leash to the 2° internal magnetic grasper (Fig. 15.8).
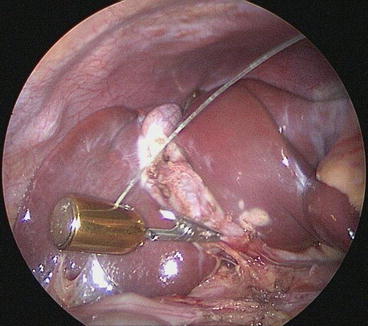
Fig. 15.8
A leash is added to the 2° internal magnetic grasper (IMANLAP Ltd) to prevent interactions produced between IDMGs. This is helpful when beginning with the practice of magnet-assisted laparoscopic surgery
Another solution to this problem is the implementation of the non-magnetic curved Williams grasper™ to replace the 2° internal magnetic grasper (The Hybrid Method).
To carry out the surgeries, the same 12-mm trocar is used and the Williams grasper™ introduced parallel to the trocar (Fig. 15.9). This facilitates the election of the most adequate fixation site for the internal magnetic grasper. When the Williams grasper™ (IMANLAP Ltd) leaves an indentation in the gallbladder, the internal magnetic grasper can be anchoraged straightforwardly. Once the fundus is retracted over the liver edge, the non-magnetic curved grasper is used to take control of movements in the already formed bassinet (Fig. 15.10). Whenever necessary a colangiography can be done by performing the puncture in the right hipocondrium (Fig. 15.11). The rest of the procedure is as described anteriorly (Fig. 15.12). The pneumoperitoneum remained stable even during the fulfillment of extreme movements (Figs. 15.13, 15.14).