Chapter 48 Benign tumors and pseudotumors of the biliary tract
Overview
Painless jaundice is most frequently caused by obstruction of the extrahepatic bile duct by malignant periampullary neoplasms, but benign tumors and pseudotumors of the biliary tract, although rare, should be included in the differential diagnosis. Benign biliary tumors are clinical rarities that in the past have been the subject of infrequent case reports, usually combined with a review of the literature. In previous series, benign bile duct tumors have been reported in 0.1% of all biliary tract operations and have constituted only 6% of all extrahepatic bile duct neoplasms (Burhans & Myers, 1971). To date, fewer than 300 cases of benign bile duct tumors have been reported in the English literature. As shown in Table 48.1, benign neoplasms are derived from the epithelia or from nonepithelial structures that make up the normal bile duct (Levy et al, 2002). Similarly, pseudotumors or tumorlike lesions of the bile duct or other periampullary tissues can cause biliary tract obstruction and jaundice. When pseudotumors or nontraumatic inflammatory strictures of the extrahepatic bile duct are included, the incidence increases, with some surgical series reporting up to a 10% to 25% incidence of benign biliary pseudotumors (Corvera et al, 2005; Koea et al, 2004). Importantly, these series demonstrate that with current preoperative staging tools, it is often impossible to distinguish between benign and malignant etiologies for biliary obstruction, so preoperative tissue confirmation does not often alter management in resectable patients.
Table 48.1 Benign Tumors and Pseudotumors that Can Cause Bile Duct Obstruction
| Epithelial Tumors |
| Nonepithelial Tumors |
| Neural Tumors |
| Pseudotumors |
Modified from Levy AD, et al, 2002: Benign tumors and tumor-like lesions of the gallbladder and extra-hepatic bile ducts: radiologic–pathologic correlation. Radiographics 22:387-413.
Biliary cystadenoma is not covered in this chapter because the lesion usually presents as an intrahepatic cystic neoplasm, which is difficult to differentiate from cystadenocarcinoma (see Chapter 79B). Indeed, benign and malignant epithelium frequently coexist, and histologic diagnosis is extremely difficult (Ishak et al, 1977; Marsh et al, 1974; Moore et al, 1984; Woods, 1981).
Embryologic And Anatomic Factors
Benign tumors of a variety of histologic types have been observed in the extrahepatic ductal system. The embryology and anatomy of the region account for this to a large degree (see Chapter 1A). Embryologically, the extrahepatic biliary tree develops in close relationship to the liver, arising from a thickened area of endoderm on the ventral surface of the primitive gastrointestinal (GI) tract at the junction of the foregut and hindgut in the 3-mm human embryo during the fifth week of intrauterine life. This small outpouching is the anlage of the liver, extrahepatic biliary ducts, gallbladder, and the ventral bud of the pancreas.
A diverticulum evolves from this thickened area, which divides into a superior and inferior bud as it grows into the ventral mesogastrium (Fig. 48.1A). The ventral pancreatic bud develops from the superior surface of the diverticulum, proximal to the enlarging terminal sacculations. The cranial sacculation, the larger of the two, pushes ventrally and cranially into the septum transversum, which separates the thoracic from the celomic cavity. Composed of a solid mass of endodermal cells, it spreads out into the substance of the septum transversum, eventually forming the right and left lobes of the liver. Cephalad growth and extension of the cranial sacculation results in stretching of the endodermal cell mass from the duodenum to the liver, which eventually evolves into the extrahepatic biliary tree. At approximately the seventh week of intrauterine life, vacuolization takes place within the solid mass of cells of the primitive extrahepatic biliary tree and results in the development of a ductal lumen.
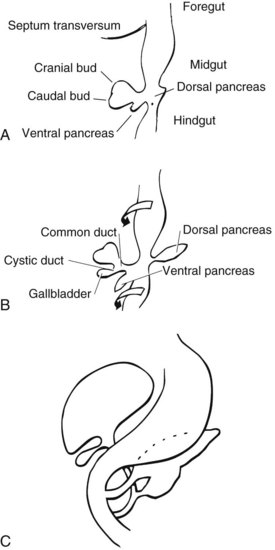
Before the 7-mm stage, the common bile duct (CBD) is attached to the ventral surface of the duodenum close to the ventral pancreatic bud. At the 7-mm stage, left-to-right rotation of the ventral pancreas and duodenum takes place so that the CBD eventually enters on the posteromedial surface of the duodenum (Fig. 48.1B and C). The gallbladder and cystic duct develop concurrently from the caudal portion of the primitive hepatic diverticulum during the same period (Lindner & Green, 1964).
The CBD lies in the right border of the hepatoduodenal ligament between serosal surfaces. The ductal wall is composed of mucosa, fibrous tissue, and serosa. Rare smooth muscle fibers may be found in the duct wall, but muscular tissue is not a prominent component. Thickness of the duct wall varies from 0.8 to 1.5 mm, with an average of approximately 1.1 mm (Mahour et al, 1967). The terminal end of the duct is invested with muscle fibers, as elegantly described by Boyden (1957). At this point the CBD usually joins with the major pancreatic duct, but they may fail to unite and enter the duodenum separately (Dowdy et al, 1961).
The mucosa lining the extrahepatic biliary tree consists of a single layer of columnar epithelium and a tunica propria containing mucous glands. Scattered chromogranin-positive cells can be formed in glands of the normal gallbladder neck, and rare cells immunoreactive for somatostatin have been found between the lining epithelium of the hepatic duct in patients with biliary disease (Dancygier et al, 1984). It has been observed that chronic inflammation of the biliary tract may result in intestinal metaplasia of the mucosa, which seems to result in an increase in the number of argentaffin cells (Kulchitsky cells). Barron-Rodriguez and colleagues (1991) have suggested that these changes may be the basis for the development of carcinoid tumors of the biliary tree. The epithelial surface of the duct is generally flat except for tiny pits in the mucosa known as sacculi of Beale, which are luminal openings for the intramural mucous glands. As the duct penetrates the wall of the duodenum, the mucosa appears to become thickened and the surface roughened by longitudinal folds of mucosa, or valvules, particularly at the terminal end of the duct. According to Boyden (1936), the valvules were first described in the Fabrica of Vesalius (1543), followed later by a more detailed description by Santorini (1724). Brown and Echenberg (1964) described a more frequent occurrence of transversally oriented flaps or valvules that face the duodenal lumen and probably function to prevent reflux of duodenal contents into the biliary tree and pancreatic ducts (Fig. 48.2). Baggenstoss (1983) has also reported that free folds of ductal epithelia in the form of papillary processes may extend 2 to 3 mm beyond the Vaterian orifice.

FIGURE 48.2 Artist’s representation of the macroscopic anatomy of the choledochoduodenal junction, depicting the transverse valvules described by Brown and Echenberg (1964), which probably serve to prevent reflux from the duodenum.
Clinical Presentations And Diagnosis
Patients with benign biliary tract tumors, and often those with inflammatory masses masquerading as neoplasms, invariably present with clinical manifestations of jaundice. The onset of icterus may be insidious or intermittent, with few other symptoms. On the other hand, the presentation may be sudden and associated with colicky epigastric pain, referred to the back or shoulder, along with nausea and vomiting. There is seldom any significant weight loss, unlike patients with pancreas cancer or cholangiocarcinoma, who frequently present with jaundice, poor appetite, and weight loss (see Chapters 50B and 58B). Because these tumors are relatively slow growing, some of the clinical symptoms may be intermittent or gradually progressive over an extended period only to culminate with obstructive jaundice. No clinical symptoms are apparent that can help the physician differentiate a benign biliary tract tumor from other, more common causes of biliary tract obstruction.
Physical findings are likewise nonspecific: liver enlargement, a palpable gallbladder, tenderness to palpation in the right hypochondrium, and jaundice. Indeed, because of the lack of characteristic symptoms and physical findings, benign biliary tumors usually are not diagnosed preoperatively or antemortem (Chu, 1950).
Reports since the early 1970s have emphasized the usefulness of percutaneous transhepatic cholangiography (PTC) and endoscopic retrograde cholangiopancreatography (ERCP) in the establishment of a preoperative diagnosis of extrahepatic obstruction and in distinguishing between calculus and tumor as a cause (see Chapter 18; Kittredge & Baer, 1975). Noninvasive imaging of the biliary tree with magnetic resonance cholangiopancreatography (MRCP) and high-quality computed tomography (CT) also now play a significant role in the diagnosis of these lesions. In their report of a patient with granular cell myoblastoma, Jain and colleagues (1979) suggested that an eccentric, short stenosis might be associated with a benign biliary tumor. However, obstructive changes identical to those seen in malignant neoplasms are not uncommon and indeed may be produced by inflammatory masses (Hadjis et al, 1985; Stamatakis et al, 1979). Although PTC and ERCP cannot distinguish between a benign tumor and a malignant process, adequate visualization of the ductal system can provide vital information concerning tumor location, extension, and size as well as the status of the intrahepatic ductal system. However, no preoperative diagnostic study is capable of reliably distinguishing benign from malignant tumorous obstruction of the biliary ducts. Endobiliary brush cytology has a high positive predictive value but, unfortunately, the negative predictive value is too low for clinical usefulness, particularly in the setting of a resectable tumor. Similarly, molecular study of cytology specimens, such as K-ras mutational analysis, has not shown improved diagnostic accuracy (Sturm et al, 1999). Newer minimally invasive tissue-acquisition techniques that include endoscopic, ultrasound-guided methods may improve diagnostic accuracy, although negative biopsy results still offer no assurances because of the suboptimal negative predictive value. Therefore these tests often do not often alter clinical management in the resectable patient (Byrne et al, 2004; Eloubeidi et al, 2004).
Papilloma And Adenoma
The most common variety of benign tumor of the extrahepatic biliary tree is that arising from the glandular epithelium lining the ducts. Roughly two thirds of the benign neoplasms reported fall into the category of either polyp, adenomatous papilloma, or adenoma. Chu (1950), in his classic review of benign biliary neoplasms, found that 26 out of 30 cases studied were either papillomas or adenomas. A similar observation was made by Dowdy and colleagues (1962), when 36 of the 43 reviewed cases were noted to be either papillomas or adenomas. Since 1962, 58 additional patients have been added to the English literature (Bahuth & Winkley, 1966; Short et al, 1971; Sull & Brown, 1972; Archie & Murray, 1978; Lukes et al, 1979; Bergdahl & Andersson, 1980; Austin et al, 1981; Gouma et al, 1984; Van Steenbergen et al, 1984; Thomsen et al, 1984; Byrne et al, 1989; Loh et al, 1994; Chae et al, 1999; Fletcher et al, 2004; Kunisaki et al, 2005; Boraschi et al, 2007; Akaydin et al, 2009). Presently, we have traced a total of 120 patients reported in the English literature with benign polyps, adenoma, or cystadenoma.
A slight female predominance (1.3 : 1) in the incidence of these lesions has been noted, and although the average age at diagnosis is 58 years, the youngest recorded occurrence was in a 3-year-old child (Wardell, 1969). Leriche (1934) reported a massive papillomatous tumor weighing 750 grams, arising from the CBD of a 4-year-old child.
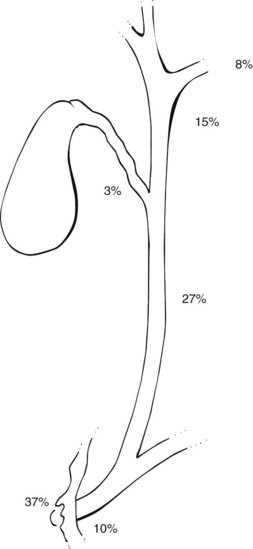
The anatomic distribution of papillomas or adenomatous lesions reported to date appears in Figure 48.3. The majority are found either in the ampulla or in close proximity to the Vaterian system (47%), and the CBD (27%) is the second most frequent site.
The onset of symptoms may vary from a few weeks to 35 years. Jaundice, a presenting symptom in more than 90% of patients (McIntyre & Pay-Zen, 1968), occurs intermittently in approximately 40% of patients. Most patients complain of right upper quadrant pain associated with the jaundice. Wright (1958) reported a patient with relapsing pancreatitis who was cured by excision of a CBD polyp that had prolapsed into the ampulla of Vater. Gallstones or biliary calculi are reported in only 20% of patients found to have benign extrahepatic ductal tumors. Cattell and Pyrtek (1950) suggest that recurrence of symptoms following cholecystectomy should suggest the possibility of a tumor in the ampullary area rather than biliary dyskinesia.
A benign adenomatous tumor should be included on the differential list in all secondary operations performed for obstruction of the biliary tree. Interestingly, Kunisaki and colleagues (2005) described the case of a 54-year-old man who showed up with abdominal pain and jaundice 3 years after a cholecystectomy for cholecystitis and choledocholithiasis. ERCP revealed impingement of the common hepatic duct (CHD) at the level of the cystic duct, without filling of the cystic duct remnant. Reexploration for a presumed diagnosis of retained cystic duct stone revealed a 2-cm papillary adenoma of the cystic duct remnant, compressing the CBD (Mirizzi syndrome; see Chapter 42B) and causing symptoms. These lesions are generally soft, difficult to palpate, and present little or no resistance to exploring ductal probes; thus they are difficult to detect at operation and are more frequently detected by intraoperative cholangiography, ultrasonography, or choledochoscopy (see Chapter 21).
The radiographic features of extrahepatic bile duct adenomas are often difficult to distinguish from cholangiocarcinomas and even ampullary cancers (see Chapters 50B and 59; Figs. 50B.2 and 50B.8). Ultrasound typically reveals a nonshadowing intraluminal mass, sometimes with a visible pedicle or stalk but more often with a sessile architecture. ERCP will show a lobulated intraluminal filling defect that is often obscured by mucin accumulation in mucin-producing adenomas. Lesions developing in the lower CBD near the ampulla may actually protrude through the papilla and be visible endoscopically, and we have seen such a case. In contrast, malignant lesions developing in the ampullary area tend to be infiltrative and are usually larger, firmer, and more likely to be ulcerated at presentation. Initial symptoms related to bleeding in association with benign adenomatous polyps of the bile ducts are exceedingly rare, although Teter (1954) recorded a death due to massive hemorrhage secondary to such a lesion.
Kozuka and colleagues (1984) suggested that most polypoid or papillary cancers of the extrahepatic duct arise from preexisting adenomas (see Chapter 50B). In a review of 43 carcinomas of the extrahepatic tree, they identified an adenomatous residue in nine (21.4%). Gouma and colleagues (1984) reported a case of intrahepatic bile duct papillomata associated with changes of nuclear atypia and reviewed the literature, suggesting that it is reasonable to regard these lesions as having low-grade malignant potential. Pathologic review of the specimens often show foci of carcinoma in situ, atypia, or dysplasia; these may point to a premalignant nature, but the rarity of such lesions makes definitive conclusions difficult.
Although it has been suggested that biliary adenomas may be the result of a focal reactive process to injury, the exact etiology remains uncertain. Miyano and colleagues (1989) demonstrated that these lesions could be produced experimentally by performing a choledochopancreatostomy in puppies, a model for anomalous choledochopancreatic ductal junction. After several years, mucosal hyperplasia was observed in 100% of the dogs, and almost half had bile duct adenomas.
Austin and colleagues (1981) reported two patients who presented with obstructive jaundice and solitary, nonparasitic liver cysts. At reoperation, the first was found to have a papillary adenoma in the CHD, which was excised; the second had an obstructing polypoid cystadenoma of the left hepatic duct compressing the right biliary system.
A possible association was proposed between solitary, nonparasitic liver cysts and adenomas of the ductal system (Austin et al, 1981), and the clinical course of these two underscores the difficulty in detection of soft adenomatous tumors obstructing the extrahepatic biliary tree. An association between nonparasitic cystic biliary disease and the development of cholangiocarcinoma has also been described in the literature (Schiewe et al, 1968; Jones & Shreeve, 1970; Gallagher et al, 1972; Dayton et al, 1983; Nasu et al, 1971; Leroy et al, 1979). However, any association between these overt malignancies and the presence of preexisting adenoma or papilloma within biliary cysts is difficult to prove.
Multiple Biliary Papillomatosis
Multiple biliary papillomatosis (MBP) is a rare disease characterized by the presence of numerous mucin-secreting papillary adenomas within the extrahepatic and/or intrahepatic biliary tree. It is generally considered a low-grade malignancy with a propensity for local recurrence after resection. Histologically, these papillomas consist of fibrovascular stalk covered by a single layer of epithelial cells with apical mucin and minimal pleomorphism (Tsui et al, 2000). The etiology and pathogenesis of MBP remain unclear. One hypothesis includes induction of mucosal metaplasia or hyperplasia in response to chronic biliary inflammation by stones, infection, or pancreatic juice. Terada (1991) and Cheng (1999) suggested a relationship between MBP and Caroli disease that may indicate a congenital etiology. Most of the reported cases are from Asia, which may reflect a racial or geographic predeliction, but such an association has not yet been established.
Preoperative diagnosis is made radiologically and may be made more frequently now, since the advent of widespread availability of endoscopic retrograde cholangiography (ERC), MRCP, and direct cholangioscopy. The endoscopic examination of the papilla of Vater often shows a widely open orifice with mucin drainage. Direct or noninvasive cholangiography shows multiple intraluminal filling defects that typically do not move with vigorous catheter irrigation and hence can be differentiated from mucin or stones. The lesions can be intrahepatic, extrahepatic, or both (D’Abrigeon, 1997). Tompkins and colleagues (1976) have emphasized the value of intraoperative endoscopy in the evaluation of the biliary tree for multiple lesions. Several studies have suggested that endoscopic ultrasound (EUS) can be at least as accurate as ERCP in diagnosing MBP, with the additional advantage of visualizing invasion of the duct wall or adjacent vessels and metastasis to locoregional lymph nodes in the presence of malignancy (Mukai, 1995; Ma, 2000; Lai, 2002).
Caroli and colleagues (1959) first reported the occurrence of diffuse papillomatosis in both the intrahepatic and extrahepatic ducts of a 42-year-old male. Although the presenting symptoms were of abdominal pain and jaundice, the patient was also noted to be anemic secondary to hemobilia. A T-tube was placed in the biliary tree, through which 10 L of mucoid secretions were drained in the first 24 hours following surgery. The patient died 48 hours later. It was noted that the biliary secretions had a high potassium content, which the authors postulated might be analogous to the mucoid diarrhea and hypokalemia associated with villous adenoma of the colon. In the same report, a second patient presented with cholangitis and was reported to be cured following a left hepatectomy for papillomatosis confined to the left intrahepatic ducts.
Since Caroli’s first report in 1959, an additional 87 cases of MBP have been reported in the English literature. A review of 78 cases by Yeung and colleagues (2003) showed a male/female ratio of approximately 2 : 1, with a mean age at presentation of 63 years (range, 6 to 83 years). The most common symptoms at the initial visit were abdominal pain and jaundice. Almost half of the patients (42%) had diffuse intrahepatic and extrahepatic disease, and 27% had only intrahepatic disease; another 27% had only extrahepatic disease, and two patients had involvement of the gallbladder. Malignant transformation was seen in 42% of the patients at the time of presentation. Only 55% of the patients were candidates for a curative resection, and the remainder were palliated in various ways, including choledochoscopic laser ablation, iridium-192 intraluminal therapy, percutaneous cholangioscopic electrocoagulation, and combined cholangioscopic laser ablation and external beam radiotherapy.
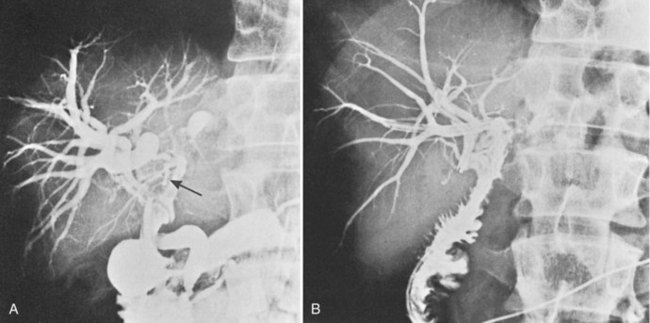
The low-grade malignant potential of MBP has been the subject of many studies. Cattell and colleagues (1962) suggested that these lesions had a low-grade malignant potential after reporting recurrence of obstructive jaundice in a patient within a year of undergoing successful placement of a T-tube. Indeed, risk of malignant transformation with nuclear atypia or carcinoma in situ is significant, and it is commonly observed in papillary lesions. Ohta and others have reported point mutations of the KRAS gene in benign papillary lesions (Ohta et al, 1993). Padfield and colleagues (1988) documented basement membrane discontinuities in three patients consistent with patterns accompanying malignant tumors; they cautioned that papillary neoplasms, although histologically benign, should be considered premalignant. Gouma and others (1984) reported a similar case, in which intrahepatic bile duct papillomata (Fig. 48.4A) were associated with changes of nuclear atypia. The patient was treated by left hepatic resection that included the base of the papillomatous lesions, and biliary-enteric continuity was established by hepaticojejunostomy to the residual right liver (Fig. 48.4B). The patient was symptom-free and without recurrence 4 years after surgery.
The authors concur with Cattell’s view that it is reasonable to regard these lesions as having low-grade malignant potential. A further patient has been reported who lived approximately 5 years before dying of cholangitis (Madden & Smith, 1974). Treatment had included partial hepatic resection, choledochoduodenostomy, and weekly courses of carmustine (BCNU). Some decrease in the amount of tumor was observed following therapy, and although cellular atypia was reported, no malignant changes could be documented at autopsy. Of the two recently reported patients, an 80-year-old male died after choledochoduodenostomy because of variceal bleeding, but the second, reported by Gertsch and colleagues (1990), was reported alive and well 15 months after curettage (Hubens et al, 1991).
The extent, distribution, and secondary obstructive changes induced by these soft lesions present management challenges. If the lesions are limited and confined to one liver lobe, liver resection should be strongly considered, although attempted radical surgery by means of hepatic lobectomy has been reported in only five cases: One of these was alive and well at 4 years (Gouma et al, 1984). One further case was reported alive 6 months after surgery with no evidence of recurrence, and one died 6 years after resection with diffuse malignant tumors in the right lobe of the liver after initial left hepatic lobectomy. The remaining two patients had multiple papillomatoses, apparently localized to the left hepatic duct at operation; both had recurrence in the common and right hepatic duct 6 months and 3 years after lobectomy and died 5 and 6 years, respectively, after the first operation. It seems clear, therefore, that even major resectional surgery for this lesion has a high recurrence rate; Gouma and colleagues (1984) were able to trace 12 patients for whom adequate follow-up figures were available and found mean survival to be 28 months. It should be noted, however, that although no patient survived more than 6 years, the only 5-year survivals were in three cases submitted to radical surgery.
A report by Helling and Strobach (1996) documents a 67-year-old female patient with papillomatosis and high-grade dysplasia occluding the left hepatic duct who was successfully managed by a left hepatic lobectomy. The patient was disease free 20 months following resection. The authors reviewed the literature and commented on three important features of this lesion: 1) a high recurrence rate, with approximately 50% of patients requiring reoperation; 2) copious mucin production that may lead to fluid electrolyte imbalances, and 3) malignant transformation, which is observed in a significant percentage of patients (Helling & Strobach, 1996). Since this report, five additional extrahepatic benign papillary lesions have been recorded (Loh et al, 1994; Lam et al, 1996; Meng et al, 1996; Khan et al, 1998; Yeung et al, 2003).
An intubational approach to papillomatosis affecting the entire biliary tree has been described (Fig. 48.5). Employment of the approach described by Hutson and colleagues (1984) and by Barker and Winkler (1984) seems reasonable: a Roux-en-Y hepaticodochojejunostomy is fashioned in such a manner as to allow a jejunal fistula for access to the biliary tree postoperatively and permit repeated curettage or intubation. Meng and colleagues (1996) reported on the use of holmium : YAG laser therapy via choledochoscopy and successful ablation after curettage; after four sessions of choledochoscopy and laser therapy, all tumor was ablated, and there were no signs of tumor recurrence at 6 months. Lastly, consideration might be given to chemotherapy, especially with agents excreted by the liver. Recently Beavers and colleagues (2001) reported the case of a 59-year-old patient with recurrent cholangitis from diffuse biliary papillomatosis that persisted even after a left hepatectomy and hepaticojejunostomy. Because of deteriorating liver function, she was placed on the list for liver transplantation and underwent successful orthotopic liver transplantation (OLT) with a Roux-en-Y hepaticojejunostomy. She was alive and asymptomatic 9 months following the surgery. Similarly, Dumortier and colleagues (2001)
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


