CHAPTER 82 Bacterial, Parasitic, and Fungal Infections of the Liver, Including Liver Abscess
Lawrence S. Friedman served as an author of this chapter on previous editions of this textbook.
The liver serves as the initial site of filtration of absorbed intestinal luminal contents and is particularly susceptible to contact with microbial antigens of all varieties. In addition to infection by viruses (see Chapters 77 to 81), the liver can be affected by (1) spread of bacterial or parasitic infection from outside the liver; (2) primary infection by spirochetal, protozoal, helminthic, or fungal organisms; or (3) systemic effects of bacterial or granulomatous infections.
BACTERIAL INFECTIONS INVOLVING OR AFFECTING THE LIVER
GRAM-POSITIVE AND GRAM-NEGATIVE BACTERIA
Toxic Shock Syndrome: Staphylococcus aureus or Group A Streptococci
Toxic shock syndrome is a multisystem disease caused by toxic shock syndrome toxins, which are superantigens that cause T cell activation and massive cytokine release. Originally described in association with serious infections caused by Staphylococcus aureus, this syndrome is now more frequently a complication of group A streptococcal infections, particularly necrotizing fasciitis.1 Risk factors for S. aureus toxic shock syndrome include tampon use and surgical wound infection. Typical findings include a scarlatiniform rash, mucosal hyperemia, hypotension, vomiting, and diarrhea.2 Hepatic involvement is almost always present and can range from elevations of serum aminotransferase levels to jaundice and extensive necrosis. Histologic findings in the liver include microabscesses and granulomas. The diagnosis is confirmed by culture of toxigenic Streptococcus pyogenes or S. aureus from the wound, blood, or other body sites. For wound infections or necrotizing fasciitis, surgical intervention is critical. Clindamycin, in conjunction with another active agent, is recommended to interfere with bacterial toxin production. Antibiotics effective against S. aureus include nafcillin for methicillin-sensitive isolates and vancomycin or linezolid for methicillin-resistant isolates, whereas penicillin remains active against S. pyogenes. Intravenous immunoglobulin may have a benefit in the setting of toxic shock associated with S. pyogenes.3
Clostridia
Clostridial myonecrosis involving Clostridium perfringens usually is a mixed anaerobic infection that results in the rapid development of local wound pain, abdominal pain, and diarrhea. The skin lesions become discolored and even bullous, and gas gangrene spreads rapidly, leading to a high mortality rate. Jaundice may develop in up to 20% of patients with gas gangrene and is predominantly a consequence of massive intravascular hemolysis caused by an exotoxin elaborated by the bacterium.4 Evidence of liver involvement may include abscess formation and gas in the portal vein. Hepatic involvement does not appear to affect mortality. The presence of clostridial bacteria portends a poor prognosis in persons with cirrhosis.5 Surgical débridement with wide excision is essential; penicillin and clindamycin are effective antibiotics.
Actinomyces
Actinomycosis is caused most commonly by Actinomyces israelii, a gram-positive anaerobic bacterium. Although cervicofacial infection is the most frequent manifestation of actinomycotic infection, gastrointestinal involvement occurs in 13% to 60% of patients.6,7 Hepatic involvement is present in 15% of cases of abdominal actinomycosis and is believed to result from metastatic spread from other abdominal sites. Common presenting manifestations of actinomycotic liver abscess include fever, abdominal pain, and anorexia with weight loss.8,9 The course is more indolent than that seen with the usual causes of pyogenic hepatic abscess and thus may be mistaken for a tumor.8 Fistula formation and invasion of other surrounding tissues such as the pleural space can occur. Anemia, leukocytosis, an elevated erythrocyte sedimentation rate, and an elevated serum alkaline phosphatase level are nearly universal. Radiographic findings are nonspecific; multiple abscesses may be seen in both lobes of the liver.
The diagnosis is based on aspiration of an abscess cavity and either visualization of characteristic sulfur granules or positive results on an anaerobic culture. Most abscesses resolve with prolonged courses of intravenous penicillin or oral tetracycline. Large abscesses can be drained percutaneously or resected surgically.10
Listeria
Hepatic invasion in adult human Listeria monocytogenes infection is uncommon. One report described thirty-four cases of listeriosis involving the liver, ranging from solitary to multiple abscesses and acute and granulomatous hepatitis.11 Hepatic histologic features include multiple abscesses and granulomas. Predisposing conditions include immunosuppression, diabetes mellitus, and underlying liver disease, including cirrhosis, hemochromatosis, or chronic hepatitis. The diagnosis of disseminated listerial infection is based on a positive culture result from blood or isolation from an aspirate in the case of a liver abscess. Treatment is with ampicillin or penicillin, often with gentamicin for synergy.12
Shigella and Salmonella
Several case reports have described cholestatic hepatitis attributable to enteric infection with Shigella.13,14 Histologic findings in the liver have included portal and periportal infiltration with polymorphonuclear neutrophils, hepatocyte necrosis, and cholestasis.
Typhoid fever, caused by Salmonella typhi, is a systemic infection that frequently involves the liver. Elevation of serum aminotransferase levels is common, whereas the serum bilirubin level may rise in a minority of cases.15 Some patients may present with an acute hepatitis-like picture, characterized by fever and tender hepatomegaly.16 Cholecystitis and liver abscess may complicate hepatic involvement with S. typhi infection.17
Hepatic damage by S. typhi appears to be mediated by bacterial endotoxin, although organisms can be visualized within the liver tissue. Endotoxin may produce focal necrosis, a periportal mononuclear infiltrate, and Kupffer cell hyperplasia in the liver. These changes resemble those seen in gram-negative sepsis. Characteristic typhoid nodules scattered throughout the liver are the result of profound hypertrophy and proliferation of Kupffer cells. The clinical course can be severe, with a mortality rate approaching 20%, particularly with delayed treatment or in patients with other complications of Salmonella infection. The suggestion has been made that severe typhoid fever with jaundice and encephalopathy can be differentiated from acute liver failure by the presence of an elevated serum alkaline phosphatase level, mild hypoprothrombinemia, thrombocytopenia, hepatomegaly, and an aspartate aminotransferase (AST) level greater than the alanine aminotransferase (ALT) level.18 Ciprofloxacin and ceftriaxone are first-line agents for the treatment of typhoid fever.
S. paratyphi A and B (Salmonella enterica serotypes paratyphi A and B) are the predominant causes of paratyphoid fever. As in typhoid fever, abnormalities in liver biochemical tests, particularly serum aminotransferase levels, with or without hepatomegaly, are common.19 Liver abscess is a rare complication.20 Treatment is with a third-generation cephalosporin or a fluoroquinolone.
Yersinia
The subacute septicemic form of the disease resembles typhoid fever or malaria. Multiple abscesses are distributed diffusely in the liver and spleen. In some cases, the occurrence of Y. enterocolitica liver abscesses may lead to the detection of underlying hemochromatosis.21,22 The mortality rate is approximately 50%. Fluoroquinolones are the preferred antibiotics.
Gonococci
In approximately 50% of patients with disseminated gonococcal infection, serum alkaline phosphatase levels are elevated, and in 30% to 40% of patients, AST levels are elevated.23 Jaundice is uncommon.
The most common hepatic complication of gonococcal infection is the Fitz-Hugh–Curtis syndrome, a perihepatitis that is believed to result from direct spread of the infection from the pelvis (see later).23 Clinically, patients describe a sudden, sharp pain in the right upper quadrant. The pain may be confused with that of acute cholecystitis or pleurisy. Most patients have a history of pelvic inflammatory disease. The syndrome is distinguished from gonococcal bacteremia by a characteristic friction rub over the liver and negative blood culture results. The diagnosis is made by vaginal culture for gonococci. The overall prognosis of gonococcal infection appears to be unaffected by the presence of perihepatitis.24 Ceftriaxone is the antibiotic of choice.
Legionella
Legionella pneumophila, a fastidious gram-negative bacterium, is the cause of Legionnaires’ disease. Although pneumonia is the predominant clinical manifestation, abnormal liver biochemical test results are frequent, with elevations in serum aminotransferase levels in 50%, alkaline phosphatase levels in 45%, and bilirubin levels in 20% of cases (but usually without jaundice). Involvement of the liver does not influence clinical outcome. Liver histologic changes include microvesicular steatosis and focal necrosis; organisms can be seen occasionally. The diagnosis is confirmed by direct fluorescence of antibody in the serum or sputum or of antigen in the urine.25 The antibiotic of choice is azithromycin or a fluoroquinolone.
Burkholderia pseudomallei (Melioidosis)
Burkholderia pseudomallei is a soil-borne and water-borne gram-negative bacterium that is found predominantly in Southeast Asia. The clinical spectrum of melioidosis ranges from asymptomatic infection to fulminant septicemia with involvement of the lungs, gastrointestinal tract, and liver. Histologic changes in the liver include inflammatory infiltrates, multiple microabscesses, and focal necrosis. Organisms can be visualized with a Giemsa stain of a liver biopsy specimen.26 With chronic disease, granulomas may be seen. Some liver abscesses may demonstrate a “honeycombing” appearance on computed tomography.27 Abscesses may need to be drained or débrided, and ceftazidime or meropenem is the initial drug of choice followed by a prolonged course of trimethoprim-sulfamethoxazole, with or without doxycycline.28
Brucella
Brucellosis may be acquired from infected pigs, cattle, goats, and sheep (Brucella suis, Brucella abortus, Brucella melitensis, and Brucella ovis, respectively) and typically manifests as an acute febrile illness. Hepatic abnormalities are seen in a majority of infected persons, and jaundice may be present in severe cases. Typically, multiple noncaseating hepatic granulomas are found in liver biopsy specimens; less often, focal mononuclear infiltration of the portal tracts or lobules is seen.29 Rarely, brucellosis also may produce hepatosplenic abscesses.30,31 The diagnosis can be made by isolation of the organism from a cultured specimen of liver tissue and is confirmed by serologic testing in combination with a history of exposure to animals. Surgical drainage may be required for management of Brucella abscesses. The combination of streptomycin and doxycycline is the most effective antimicrobial therapy.
Coxiella burnetii (Q Fever)
Infection by Coxiella burnetii, typically acquired by inhalation of animal dusts, causes the clinical syndrome of Q fever, which is characterized by relapsing fevers, headache, myalgias, malaise, pneumonitis, and culture-negative endocarditis. Liver involvement is common.32 The predominant abnormality is an elevated serum alkaline phosphatase level, with minimal elevations of AST or bilirubin levels. The histologic hallmark in the liver is the presence of characteristic fibrin ring granulomas. The diagnosis is confirmed by serologic testing for complement-fixing antibodies.33 Treatment with doxycycline usually is effective.
Bartonella (Oroya Fever)
Endemic to Colombia, Ecuador, and Peru, Bartonella bacilliformis is a gram-negative coccobacillus that causes an acute febrile illness accompanied by jaundice, hemolysis, hepatosplenomegaly, and lymphadenopathy. Centrilobular necrosis of the liver and splenic infarction may occur. As many as 40% of patients die of sepsis or hemolysis. Prompt treatment with chloramphenicol in combination with penicillin, clindamycin, or trimethoprim-sulfamethoxazole prevents fatal complications.34
Bacillary Angiomatosis and the Acquired Immunodeficiency Syndrome
Bacillary angiomatosis is an infectious disorder that primarily affects persons with the acquired immunodeficiency syndrome (AIDS) or other immunodeficiency states. The causative agents have been identified as the gram-negative bacilli Bartonella henselae and, in some cases, Bartonella quintana.35 Infection frequently is associated with exposure to cats.
Bacillary angiomatosis is characterized most commonly by multiple blood-red papular skin lesions, but disseminated infection with or without skin involvement also has been described.36 The causative bacilli can infect liver, lymph nodes, pleura, bronchi, bones, brain, bone marrow, and spleen. Additional manifestations include persistent fever, bacteremia, and sepsis. Hepatic infection should be suspected when serum aminotransferase levels are elevated in the absence of other explanations.
Hepatic infection in persons with bacillary angiomatosis may manifest as peliosis hepatis, or blood-filled cysts (see Chapter 83). Histologically, peliosis in patients with AIDS is characterized by an inflammatory myxoid stroma containing clumps of bacilli and dilated capillaries surrounding the blood-filled peliotic cysts. Increasingly, diagnosis of Bartonella infection is by polymerase chain reaction (PCR)-based methods.37 Bacillary angiomatosis responds uniformly to therapy with erythromycin. For visceral infection, prolonged treatment with erythromycin or doxycycline should be administered.38
Bacterial Sepsis and Jaundice
Jaundice may complicate systemic sepsis caused by gram-negative or gram-positive organisms. Exotoxins and endotoxin liberated in overwhelming infection can directly or indirectly, through cytokines such as tumor necrosis factor-α (TNF-α), inhibit the transport of bile acids and other organic anions across the hepatic sinusoidal and bile canalicular membranes, thereby leading to intrahepatic cholestasis (see Chapter 20).39 Serum bilirubin levels can reach 15 mg/dL or higher. The magnitude of the jaundice does not correlate with mortality. Results of cultures of liver biopsy specimens usually are negative.
CHLAMYDIA
Fitz-Hugh–Curtis Syndrome
Although perihepatitis was first associated with gonococcal salpingo-oophoritis (see earlier), it is now most frequently associated with Chlamydia trachomatis infection.40 The presentation is similar to perihepatitis caused by gonococcal infection, with right upper quadrant pain accompanying a urogenital infection such as pelvic inflammatory disease. The diagnosis can be made by direct visualization at laparoscopy or laparotomy and supported by pathologic demonstration of endometritis, salpingitis, and microbiologic detection of C. trachomatis in the genital tract. Liver biochemical test results are generally normal. The treatment of choice is a single dose of azithromycin or seven days of doxycycline.
RICKETTSIA
Rocky Mountain Spotted Fever
Mortality from Rocky Mountain spotted fever, a systemic tick-borne rickettsial illness, has decreased considerably as a result of prompt recognition of the classic maculopapular rash in association with fever and an exposure history. A small subset of patients, however, present with multiorgan manifestations and have a high mortality rate.41 A characteristic severe vasculitis develops in these patients and is believed to be the result of a microbe-induced coagulopathy. Hepatic involvement is frequent in multiorgan disease. In one postmortem study, rickettsiae were identified in the portal triads of eight of nine fatal cases. Portal tract inflammation, portal vasculitis, and sinusoidal erythrophagocytosis were consistent findings, but hepatic necrosis was negligible. The predominant clinical manifestation was jaundice; elevations of serum aminotransferase and alkaline phosphatase levels varied. Jaundice probably results from a combination of inflammatory bile ductular obstruction and hemolysis and is associated with increased mortality.32,42
Ehrlichia
Ehrlichiae are rickettsiae that parasitize leukocytes. In the United States, human monocytic ehrlichiosis is caused principally by Ehrlichia chaffeensis and, less often, by Ehrlichia canis. Human granulocytic anaplasmosis (formerly known as human granulocytic ehrlichiosis) is caused by Anaplasma phagocytophilum.32,43 In contrast with Rocky Mountain spotted fever, a rash is often absent. Hepatic involvement is seen in greater than 80% of cases, usually in the form of mild, transient serum aminotransferase elevations. More marked aminotransferase elevations may occur occasionally, in association with cholestasis, hepatosplenomegaly, and liver failure. Liver injury is attributable to proliferation of organisms within hepatocytes and provocation of an immune response. Focal necrosis, fibrin ring granulomas, and cholestatic hepatitis can be observed. A mixed portal tract infiltrate and lymphoid sinusoidal infiltrate usually are seen. The disease generally resolves with appropriate antibiotic therapy with doxycycline.44
SPIROCHETES
Leptospirosis
Anicteric leptospirosis accounts for more than 90% of cases and is characterized by a biphasic illness. The first phase begins, often abruptly, with viral illness-like symptoms associated with fever, leptospiremia, and conjunctival suffusion, which serves as an important diagnostic clue. Following a brief period of improvement, the second phase in 95% of cases is characterized by myalgias, nausea, vomiting, abdominal tenderness, and, in some cases, aseptic meningitis.45 During this phase, a few patients have elevated serum aminotransferase and bilirubin levels with hepatomegaly.
Weil’s syndrome is a severe icteric form of leptospirosis and constitutes 5% to 10% of all cases. The first phase of this illness often is marked by jaundice, which may last for weeks. During the second phase, fever may be high, and hepatic and renal manifestations predominate. Jaundice may be marked, with serum bilirubin levels approaching 30 mg/dL (predominantly conjugated). Serum aminotransferase levels usually do not exceed five times the upper limit of normal.46 Acute tubular necrosis often develops and can lead to renal failure, which may be fatal. Hemorrhagic complications are frequent and are the result of capillary injury caused by immune complexes.45 Spirochetes are seen in renal tubules in a majority of autopsy specimens but rarely are found in the liver. Hepatic histologic findings generally are nonspecific and do not include necrosis. Altered mitochondria and disrupted membranes in hepatocytes on electron microscopy suggest the possibility of a toxin-mediated injury.
Syphilis
Secondary Syphilis
Liver involvement is characteristic of secondary syphilis.47 The frequency of hepatitis in secondary syphilis ranges from 1% to 50%.47,48 Symptoms and signs usually are nonspecific, including anorexia, weight loss, fever, malaise, and sore throat. A characteristic pruritic maculopapular rash involves the palms and soles. Jaundice, hepatomegaly, and tenderness in the right upper quadrant are less common. Almost all patients exhibit generalized lymphadenopathy. Biochemical testing generally reveals low-grade elevations of serum aminotransferase and bilirubin levels, with a disproportionate elevation of the serum alkaline phosphatase level; isolated elevation of the alkaline phosphatase is common.49 Proteinuria may be present.
Histologic examination of the liver in syphilitic hepatitis generally discloses focal necrosis in the periportal and centrilobular regions. The inflammatory infiltrate typically includes polymorphonuclear neutrophils, plasma cells, lymphocytes, eosinophils, and mast cells.47,48 Kupffer cell hyperplasia may be seen, but bile ductule injury is rare. Granulomas may be seen. Spirochetes may be demonstrated by silver staining in as many as 50% of patients. Resolution of these findings without sequelae follows treatment with penicillin.
Tertiary (Late) Syphilis
Tertiary syphilis is now rare. Although hepatic lesions are common in late syphilis, most patients are asymptomatic. Some patients describe anorexia, weight loss, fatigue, fever, or abdominal pain. The characteristic hepatic lesion in tertiary syphilis is the gumma, which can be single or multiple. It is necrotic centrally, with surrounding granulation tissue consisting of a lymphoplasmacytic infiltrate and endarteritis; exuberant deposition of scar tissue may occur, giving the liver a lobulated appearance (hepar lobatum). If hepatic involvement is unrecognized, hepatocellular dysfunction and portal hypertension with jaundice, ascites, and gastroesophageal varices can ensue. Hepatic gummas may resolve after therapy with penicillin.50
Lyme Disease
Lyme disease is a multisystem disease caused by the tick-borne spirochete Borrelia burgdorferi. Predominant manifestations are dermatologic, cardiac, neurologic, and musculoskeletal. Hepatic involvement has been described. Among 314 patients, abnormal liver biochemical test results with generally increased serum aminotransferase and lactate dehydrogenase levels were seen in 19%.51 Clinical findings included anorexia, nausea and vomiting, weight loss, right upper quadrant pain, and hepatomegaly, usually within days to weeks of the onset of illness and often accompanied by the sentinel rash, erythema migrans.52
In early stages of the illness, the spirochetes are believed to disseminate hematogenously from the skin to other organs, including the liver.53 One report has suggested that the Lyme spirochete also can cause acute hepatitis as a manifestation of reactivation,54 although the possibility of reinfection cannot be fully excluded. Histologic examination of the liver in Lyme hepatitis reveals hepatocyte ballooning, marked mitotic activity, microvesicular fat, Kupffer cell hyperplasia, a mixed sinusoidal infiltrate, and intraparenchymal and sinusoidal spirochetes.53
The diagnosis of Lyme disease is confirmed with serologic studies in patients with a typical clinical history. Hepatic involvement tends to be more frequent in disseminated disease but does not appear to affect overall outcome, which is excellent in primary disease after institution of treatment with oral doxycycline, amoxicillin, clarithromycin, or azithromycin.55 Ceftriaxone is the drug of choice for late disease.44,53
TUBERCULOSIS AND OTHER MYCOBACTERIA
Granulomas are found in liver biopsy specimens in approximately 25% of persons with pulmonary tuberculosis and 80% of those with extrapulmonary tuberculosis. Tuberculous granulomas can be distinguished from sarcoid granulomas by central caseation, acid-fast bacilli, and the presence of fewer granulomas, with a tendency to coalesce.56 Multiple granulomas in the liver also may be seen following vaccination with bacille Calmette-Guérin, especially in persons with an impaired immune response. Patients with multiple granulomas caused by tuberculosis rarely have clinically significant liver disease. Occasionally, tender hepatomegaly is found. Jaundice with elevated serum alkaline phosphatase levels may occur in miliary infection. The treatment of tuberculous granulomatous disease of the liver is the same as that for active pulmonary tuberculosis—namely, four-drug therapy.56 Hepatic involvement in Mycobacterium avium complex infection is discussed in Chapter 33.
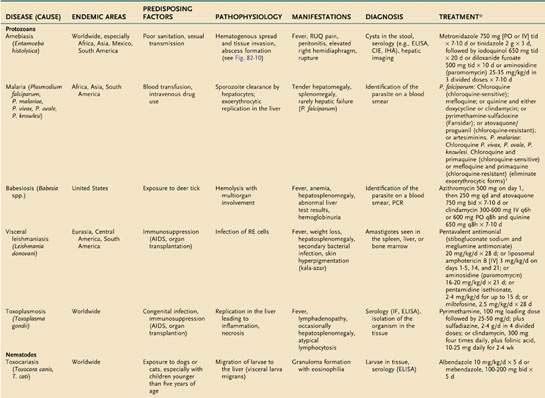
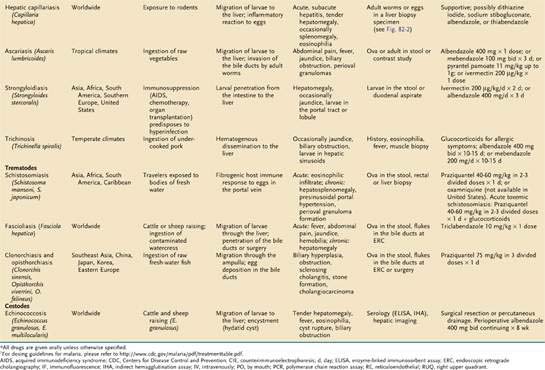
PARASITES (Tables 82-1 and 82-2)
Table 82-1 Parasitic Infections of the Liver and Biliary Tract: Classification by Pathologic Process
| PATHOLOGIC PROCESS | DISEASES |
|---|---|
| Liver Disease | |
| Granulomatous hepatitis | Capillariasis |
| Fascioliasis | |
| Schistosomiasis | |
| Strongyloidiasis | |
| Toxocariasis | |
| Portal fibrosis | Schistosomiasis |
| Hepatic abscess or necrosis | Amebic abscess |
| Toxoplasmosis | |
| Cystic liver disease | Echinococcosis |
| Peliosis hepatis | Bacillary angiomatosis |
| Reticuloendothelial Disease | |
| Kupffer cell infection or hyperplasia | Babesiosis |
| Malaria | |
| Toxoplasmosis | |
| Visceral leishmaniasis | |
| Biliary Tract Disease | |
| Cholangitis | Clonorchiasis/opisthorchiasis |
| Fascioliasis | |
| Biliary hyperplasia | Ascariasis |
| Clonorchiasis | |
| Cryptosporidiosis | |
| Fascioliasis | |
| Cholangiocarcinoma | Clonorchiasis/opisthorchiasis |
PROTOZOA (see also Chapter 109)
Malaria
An estimated 300 to 500 million persons in more than 100 countries are infected with malaria each year. The liver is affected during two stages of the malarial life cycle: first in the pre-erythrocytic phase, and then in the erythrocytic phase, which coincides with clinical illness. The life cycle of the prototypical malarial parasite is illustrated in Figure 82-1.
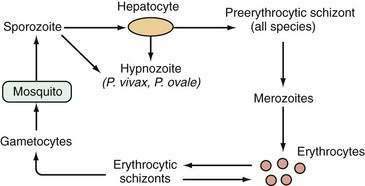
Pathobiology of the Plasmodium Life Cycle
Malarial sporozoites injected by an infected mosquito circulate to the liver and enter hepatocytes. Maturation to schizonts ensues. When the schizont ruptures, merozoites are released into the bloodstream, where they enter erythrocytes. The major species of Plasmodium responsible for malaria differ with respect to the number of merozoites released and the maturation times. Infection by Plasmodium falciparum and Plasmodium malariae is not associated with a residual liver stage after the release of merozoites, whereas infection by Plasmodium vivax and Plasmodium ovale is associated with a persistent exoerythrocytic stage, the hypnozoite, which persists in the liver and, when activated, can divide and mature into schizont forms. Plasmodium knowlesi has been identified as a fifth species capable of infecting humans and occasionally results in severe manifestations including jaundice, hepatic dysfunction, and acute kidney injury.57
The extent of hepatic injury varies with the malarial species (most severe with P. falciparum) and the severity of infection. Unconjugated hyperbilirubinemia most commonly is seen as a result of hemolysis, but hepatocellular dysfunction is also possible, leading to conjugated hyperbilirubinemia. Moderate elevations of serum aminotransferase and 5′-nucleotidase levels may be observed.58 Synthetic dysfunction (e.g., prolongation of the prothrombin time, hypoalbuminemia) may be seen as well. In severe falciparum malaria, hypoglycemia and lactic acidosis are late and life-threatening complications.59 Reversible reductions in portal venous blood flow have been described during the acute phase of falciparum malaria, presumably as a consequence of micro-occlusion of portal venous branches by parasitized erythrocytes.59
Histopathologic Features
In acute falciparum malaria in a previously unexposed person, hepatic macrophages hypertrophy, and large quantities of malarial pigment (the result of hemoglobin degradation by the parasite) accumulate in Kupffer cells, which phagocytose parasitized and unparasitized erythrocytes.60 Histopathologic features include Kupffer cell hyperplasia with pigment deposition and a mononuclear infiltrate. Hepatocyte swelling and centrizonal necrosis may be seen. All abnormalities are reversible with treatment.
Clinical Features
Only the erythrocytic stage of malaria is associated with clinical illness. Symptoms and signs of acute infection typically develop 30 to 60 days following exposure and include fever, which often is hectic, malaise, anorexia, nausea, vomiting, diarrhea, and myalgias. Jaundice caused by hemolysis is common in adults, especially in heavy infection with P. falciparum. In general, hepatic failure is seen only in association with concomitant viral hepatitis or with severe P. falciparum infection.61,62 One series identified evidence of hepatic encephalopathy in 15 of 86 patients with falciparum malaria and jaundice; four cases were fatal.61 Tender hepatomegaly with splenomegaly is common. Cytopenias are common in acute infection. The differential diagnosis includes viral hepatitis, gastroenteritis, amebic liver abscess, yellow fever, typhoid, tuberculosis, and brucellosis.
Diagnosis
The diagnosis of acute malaria rests on the clinical history, physical examination, and identification of parasites on peripheral thin and thick blood smears. Because the number of parasites in the blood may be small, repeated smear examinations should be performed by an experienced examiner when the index of suspicion is high. P. knowlesi may resemble P. malariae in morphology, and PCR-based tests may help distinguish these two species.57 Rapid antigen detection assays are available but are less reliable than other diagnostic approaches.63
Treatment
The treatment of acute malaria depends on the species of parasite and, for falciparum infection, the pattern of chloroquine resistance. Chloroquine generally is effective in areas endemic for chloroquine-sensitive species. Resistant falciparum infections can be treated with mefloquine alone; quinine and either doxycycline or clindamycin; pyrimethamine-sulfadoxine (Fansidar); a combination of atovaquone and proguanil; or artemisinin derivatives including artemisinin, artemether, and artesunate.64 For P. vivax and P. ovale infections, the addition of primaquine (in persons without glucose-6-phosphate dehydrogenase deficiency) to chloroquine or mefloquine is indicated to eliminate the exoerythrocytic hypnozoites in the liver.65
Hyperreactive Malarial Splenomegaly (Tropical Splenomegaly Syndrome)
In endemic areas, repeated exposure to malaria may lead to an aberrant immunologic response characterized by overproduction of B lymphocytes, circulating malarial antibody, and increased levels of circulating immune complexes, resulting in dense hepatic sinusoidal lymphocytosis and stimulation of the reticuloendothelial cell system. The clinical picture includes massive splenomegaly, markedly elevated antimalarial antibody levels, and high serum immunoglobulin M (IgM) levels. Severe debilitating anemia caused by hypersplenism, especially in women of childbearing age, can result.66 Variceal bleeding is uncommon but may result from portal hypertension consequent to markedly increased splenic and portal venous blood flow. Treatment consists of lifelong antimalarial therapy and blood transfusions.
Babesiosis
Babesiosis, caused by Babesia species, is a malaria-like illness transmitted by the deer tick Ixodes scapularis.67 The disease is endemic to coastal areas of the Northeast and areas of the Midwest in the United States. Clinical features include fever, anemia, mild hepatosplenomegaly, abnormalities on liver biochemical tests, hemoglobinuria, and hemophagocytosis on bone marrow biopsy specimen. The disease is especially severe in asplenic and immunocompromised patients. In rare cases, marked pancytopenia occurs. Hepatic involvement reflects the severity of the systemic illness but generally is not severe. Uncomplicated cases are treated with a combination of the following active agents: (1) oral azithromycin, 500 mg single dose followed by 250 mg once daily, plus atovaquone, 750 mg twice daily, for 7 to 10 days; or (2) oral clindamycin, 600 mg three times daily, in combination with quinine, 650 mg three times daily, for 7 to 10 days. In severe cases, the clindamycin may be given intravenously and partial or complete exchange transfusion should be considered.44
Leishmaniasis
Visceral leishmaniasis is caused by Leishmania donovani and is endemic in the Mediterranean, central Asia, the former Soviet Union, the Middle East, China, India, Pakistan, Bangladesh, Africa, Central America, and South America.68 This entity should be considered in returning travelers and military personnel from these areas. Amastigotes are ingested by the sand fly (Lutzomyia in the New World, Phlebotomus in the Old World) and become flagellated promastigotes. Following injection into the human host, the promastigotes are phagocytosed by macrophages in the reticuloendothelial system, where they multiply.
Histopathologic Features
In visceral leishmaniasis, organisms usually can be found in mononuclear phagocytes of the liver, spleen, bone marrow, and lymph nodes. Proliferation of Kupffer cells often is seen, and amastigotes (Leishman-Donovan bodies) can be detected within these cells.69 Occasionally, parasite-bearing cells aggregate within noncaseating granulomas.70 Hepatocyte necrosis can range in degree from mild to severe. Healing is accompanied by fibrous deposition, and occasionally the liver takes on a cirrhotic appearance. Nevertheless, complications of chronic liver disease are rare.
Clinical Features
Physical findings include hepatomegaly, massive splenomegaly, jaundice or ascites in severe disease, generalized lymphadenopathy, and muscle wasting.71 Cutaneous gray hyperpigmentation, which prompted the name kala-azar (black fever), is characteristically seen in patients in India. Oral and nasopharyngeal nodules resulting from granuloma formation also may be seen.
Diagnosis
The diagnosis is based on the history, physical examination, and microscopic demonstration of amastigotes by a Wright or Giemsa stain of affected tissue samples. The highest yield (90%) comes from aspiration of the spleen. Liver biopsy is less risky and associated with a yield nearly as great as that of splenic aspiration. The yield of bone marrow aspirates is 80%, and that of lymph node aspirates is 60%.54 Culture requires specialized media and may take several weeks. Serologic testing (enzyme-linked immunosorbent assay [ELISA], immunofluorescence, direct agglutination) can be used to support a presumptive diagnosis of visceral leishmaniasis but is insensitive, particularly in immunocompromised hosts.72 The leishmanin skin test (Montenegro test) is not helpful in acute visceral disease. PCR-based testing of blood or other tissue may also be useful for diagnosis as well as monitoring.73
Treatment
Pentavalent antimonial compounds are the drugs of choice for all forms of leishmaniasis. Parenteral sodium stibogluconate and meglumine antimoniate are available through the Centers for Disease Control and Prevention for treatment of infections in the United States. Treatment with antimonials should be administered for at least four weeks. Alternative parenteral agents include liposomal amphotericin B and aminosidine (paromomycin).74 Patients with AIDS and leishmaniasis often fail to respond to or relapse following treatment with conventional regimens.72 Miltefosine, a phosphocholine analog administered orally, has shown promise in visceral leishmaniasis, with a reported cure rate of 82% to 97%.75,76
Toxoplasmosis
Toxoplasmosis, caused by Toxoplasma gondii, is found worldwide. In the United States, serologic surveys suggest that exposure to T. gondii has decreased from 14% to 9% among persons ages 12 to 49.77 The infection may be transmitted congenitally or occur as an opportunistic infection that causes cerebral mass lesions in patients with AIDS. Oocysts of T. gondii in soil, water, or contaminated meat are ingested and mature in the intestinal tract of humans to become sporozoites, which penetrate the intestinal mucosa, become tachyzoites, and circulate systemically, invading a wide array of cell types.78 Hepatic involvement has been observed in severe, disseminated infection.
Clinical Features
Although most primary infections are asymptomatic, acquired toxoplasmosis can manifest as a mononucleosis-like illness with fever, chills, headache, and regional lymphadenopathy.79 Hepatomegaly, splenomegaly, and minimal elevations of serum aminotransferase levels are uncommon findings.80,81 Infections of immunocompromised hosts can result in pneumonia, myocarditis, encephalitis, and, rarely, hepatitis.78,82 Toxoplasmosis can produce atypical lymphocytosis, an otherwise unusual feature of parasitic disease.
Diagnosis
The diagnosis is best made by detecting specific IgM or IgG antibody using highly specific indirect immunofluorescence or an enzyme immunoassay.83 Specialized histologic staining techniques and tissue culture systems can provide adjunctive diagnostic support. PCR analysis of serum and liver also can be helpful in ambiguous cases.84
Treatment
Antibiotic therapy should be administered to all persons with severe symptomatic infection and to immunocompromised or pregnant patients with acute uncomplicated infection. Treatment consists of a combination of pyrimethamine and sulfadiazine, plus folinic acid to minimize hematologic toxicity, for two to four weeks.78








