Second Step—Abdominal Wall
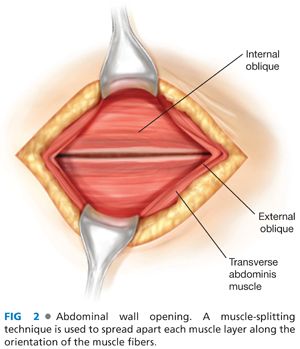
■ There are three muscle layers in the lateral abdominal wall. As these are encountered when entering the abdomen, these are the external oblique, the internal oblique, and the transversus abdominis muscles.
■ Each muscle aponeurosis is cut in the direction of the muscle fibers.
■ A muscle-splitting technique is used to spread apart each muscle layer along the orientation of the muscle fibers (FIG 2) until the peritoneum is reached.
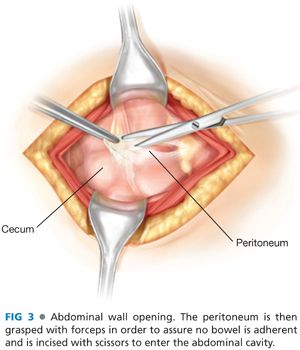
■ The peritoneum is then grasped with forceps in order to assure no bowel is adherent and is incised with scissors to enter the abdominal cavity (FIG 3).
■ An appropriate retractor is placed to enhance operative exposure. This can be either a Balfour or a Bookwalter retractor.
Third Step—Exposure of the Appendix
■ After the peritoneum is entered, the cecum is identified. Sponge sticks can be helpful to sweep the small bowel in a lateral to medial direction in order to expose the cecum.
■ Once the cecum is identified, the anterior taenia is identified. The cecum is then mobilized, following the anterior taenia to its confluence with the appendiceal base (FIG 4).
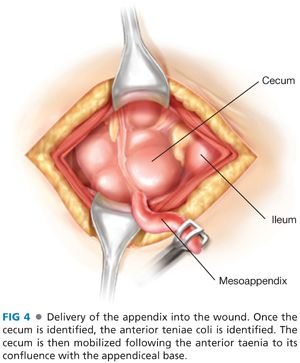
■ The convergence of all three teniae coli allows for the correct identification of the base of the appendix. This is critical to ensure that the entire appendix is removed.
■ Failure to remove the base of the appendix may cause a closed loop obstruction between a persistent fecalith at the base of the appendix and the stump staple line. This may lead to an appendiceal stump blowout postoperatively.
■ In cases of retrocecal appendicitis, the cecum will need to be fully mobilized in a lateral to medial fashion so that it is completely reflected from the retroperitoneum in order to find the appendix.
Fourth Step—Ligation and Resection
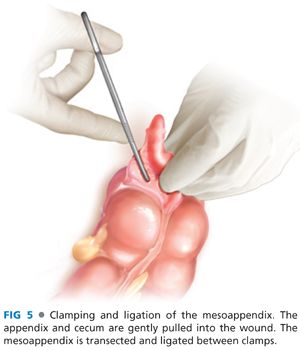
■ The appendix and cecum are gently pulled into the wound. The mesoappendix is transected and ligated between clamps (FIG 5).
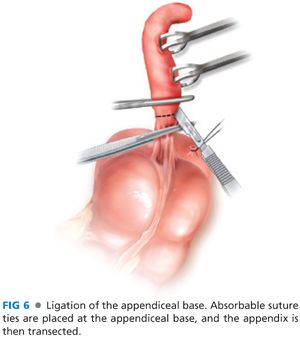
■ Absorbable suture ties are placed at the appendiceal base, and the appendix is then transected (FIG 6). There is no supporting data for electrocautery ablation of the appendiceal mucosa at the ligated stump, and this common practice clearly puts at risk the security of the suture used to ligate the appendiceal stump.
■ Inversion of the appendiceal stump may be performed if the surgeon desires. Commonly, a “Z-stitch” is used for this purpose (FIG 7).
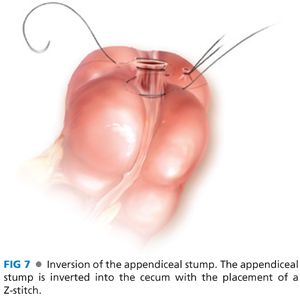
■ In the Z-stitch, the upper bite is placed as a Lembert suture and then brought below the base of the appendiceal stump and a second seromuscular stitch is placed. The base of the appendix is then inverted using forceps and the ends of the suture tied down over the inverted stump (FIG 7).
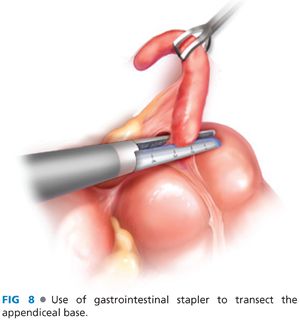
■ In cases of severe appendiceal stump edema and inflammation, a gastrointestinal stapler may be used to transect the base of the appendix, even including a segment of healthy cecal base in the resection; be careful to avoid impingement of the ileocecal valve when firing the stapler (FIG 8).
■ Irrigation of the surgical field is of unclear benefit. There are limited data in adults. A randomized prospective study in children failed to show any change in intraabdominal abscess whether irrigation was used or not used.3
Fifth Step—Closure
■ All three muscle layers are closed separately with running absorbable suture.
■ The skin can be closed, left open, or loosely approximated, depending on the severity of contamination encountered during the case.
■ For gangrenous or perforated appendicitis, considered delayed primary closure or placement of a negative pressure wound therapy device to minimize superficial surgical site infection.
■ No drain is indicated in simple appendicitis. Drain placement in cases of complicated appendicitis is also not supported by clinical trials.
OPEN APPENDECTOMY FOR APPENDICEAL NEOPLASMS
■
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


