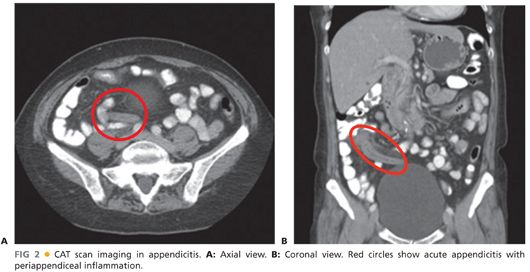
■ Computerized axial tomography (CAT; FIG 2) scan, with a 94% sensitivity and a 95% specificity, has been shown to be the most accurate imaging study for the diagnosis of acute appendicitis but is expensive and may delay surgical intervention.
■ Magnetic resonance imaging (MRI) is reserved for patients who cannot be exposed to radiation, such as pregnant women suspected of having appendicitis.
SURGICAL MANAGEMENT
Indications
■ Same indications than for open appendectomy
■ Any patient with diagnosis of appendicitis who can tolerate pneumoperitoneum and general anesthesia, provided that trained staff and the necessary equipment for a safe procedure are available
Preoperative Planning
■ Appropriate prophylactic antibiotic should be administered 30 minutes before surgery.
■ Decompression of the bladder by voiding before surgery or by using a Foley catheter may avoid injury of the bladder during trocar placement.
Patient and Team Positioning
■ The patient is secured to the table with the arms padded and tucked to the side.
■ The surgeon and the camera operator stand on the patient’s left side (FIG 3).
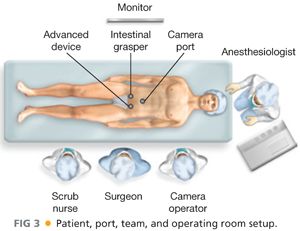
■ The monitor is placed in front of the surgeon (at eye level) on the patient’s right side.
Port Placement
■ A traditional laparoscopic appendectomy is performed using a three-port system (FIGS 3 and 4). The surgeon should be able to work two-handed.
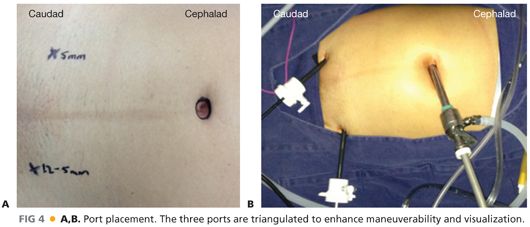
■ The ports are triangulated to enhance maneuverability and exposure.
■ A 10-mm Hasson trocar is inserted in the umbilicus. This trocar will be used for CO2 insufflation and also as a camera port.
■ A 12-mm trocar is inserted in the left lower quadrant. In addition to being the main dissection port, this port will be used for the stapler and also as an extraction site. If a good quality 5-mm camera is available, then a 5-mm port can be inserted in this location; in this alternative setup, the specimen would be retrieved through the umbilical port site.
■ A 5-mm trocar is inserted in the right lower quadrant. This trocar will be used to help retract and expose. Placement of a urinary catheter may be required before introducing the lower abdominal trocars in order to reduce the risk of bladder perforation during this step of the procedure.
TECHNIQUES
STEP 1. EXPOSURE OF THE APPENDIX AND IDENTIFICATION OF THE APPENDICEAL BASE
■ The patient is placed in a Trendelenburg position and rotated with the right side up to help mobilize the small bowel out of the field of view and to enhance operative exposure.
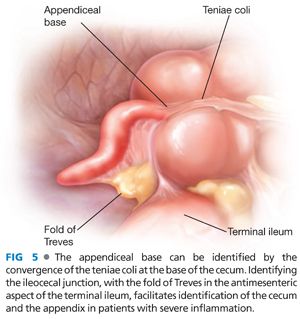
■ The fold of Treves (an antimesenteric fat fold also known as the sail sign) allows for identification of the terminal ileum (FIG 5). Following the terminal ileum distally to the ileocecal junction facilitates identification of the cecum. The appendix can usually be seen at the base of the cecum.
■ In retrocecal appendicitis cases, the cecum may have to be mobilized medially by transecting its lateral peritoneal attachments in order to expose the appendix.
■ The base of the inflamed appendix is localized by identifying the convergence of the three teniae coli at the base of the cecum (FIG 5).
STEP 2. DIVISION OF THE MESOAPPENDIX
■
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


