Chapter 104 Aneurysm and arteriovenous fistula of the liver and pancreatic vasculature
Overview
Traumatic injuries to the hepatic pedicle generally occur in conjunction with injuries to the liver or pancreas. Hemorrhage or hematoma at the porta hepatis can be indicative of injury to the hepatic artery, portal vein, or both. In blunt trauma, injury is often secondary to compression or shearing forces and disruption at the points of maximal fixation, where the porta hepatis is relatively fixed to the retroperitoneum. An isolated pedicle injury may occur with penetrating trauma, which may involve intrahepatic or extrahepatic vessels with disruption of any structure in the trajectory; see Chapters 102 and 103 for further discussion on traumatic injuries.
Vascular control can be attempted using the Pringle maneuver (1908) or by clamping the porta hepatis; this controls arterial and portal vein hemorrhage from the liver. Continuing hemorrhage is due to retrograde bleeding from the vena cava or hepatic veins. Kocherization of the duodenum and head of the pancreas by dividing the peritoneum along the lateral border of the duodenum allows for better exposure (see Chapter 63A). This maneuver is especially useful for distal pedicle injuries or those to the retropancreatic portion of the portal vein.
In cases of severe injury, hepatic arterial ligation can be used in the operating room or with the aid of angiography; this should be considered if the patient has a noticeable decrease in bleeding after the Pringle maneuver is performed. Complete selective hepatic arterial ligation is used in approximately 1% of patients (David et al, 2000). Disruption of the right or left hepatic artery may be treated by ligation, providing the ipsilateral portal vein is intact. Simple lacerations of the common hepatic artery may be repaired primarily, but blind placement of sutures should be avoided because of the proximity of the common bile duct and potential for iatrogenic injury. With vascular injuries to the pedicle, common bile duct injury should be suspected, and a cholangiogram should be performed. If right or common hepatic artery ligation is performed, or if injury to the common bile duct is evident, a cholecystectomy should be performed.
Injuries to the portal vein are difficult to manage because of profuse bleeding and the relative inaccessibility of the portal vein owing to its posterior position in the porta hepatis. These injuries are associated with a 50% to 70% mortality rate and carry a high risk of other vascular injuries (Asensio et al, 2007; Buckman et al, 2001; Coimbra et al, 2004; Fraga et al, 2009; Pearl et al, 2004). Shock or systolic blood pressure below 90 mm Hg is a significant predictor of survival, and 90% of injuries to the portal vein are caused by penetrating trauma; the most common location of injury is within the hepatoduodenal ligament. The three classifications of portal vein injuries are type A, less than 50% of vein circumference is disrupted; type B, disruption is greater than 50%; type C, complete transection is evident (Coimbra et al, 2004).
Primary venorrhaphy is the preferred approach for repair of portal vein injuries in the stable patient (Fraga et al, 2009; Pearl et al, 2004). The hemodynamic status of the patient generally determines the complexity of the repair. Other alternatives are end-to-end anastomosis, portocaval shunt, graft interpostition, vein patch graft, and portal vein ligation (Coimbra et al, 2004; Fraga et al, 2009; Pearl et al, 2004; Stone et al, 1982). Portal vein ligation can be performed only if the hepatic artery is intact, and it is an appropriate damage control option in an unstable and coagulopathic patient. Portal vein ligation has been reported with a 50% to 80% survival rate and low incidences of subsequent portal hypertension (Coimbra et al, 2004; Stone et al, 1982). Following ligation of the portal vein or superior mesenteric vein (SMV), bowel will become edematous with areas of ischemia. Most surgeons would recommend temporary abdominal closure followed by a second-look laparotomy in 48 to 72 hours. Injury to both the hepatic artery and portal vein are rare and technically difficult to manage, and at least one of these structures must be repaired to avoid hepatic necrosis.
SMV injuries are uncommon but devastating; this is due to the difficulty in obtaining exposure and getting control of hemorrhage quickly. Primary venorrhaphy is the preferred repair, when such is possible; although ligation of the SMV has been performed with variable success, it should be reserved for use in the hemodynamically unstable patient (Asensio et al, 2000, 2007). It should also be noted that superior mesenteric venous injuries are often associated with portal vein and other vascular injuries (Asensio et al, 2007).
Hepatic Artery Aneurysms and Pseudoanerysms
Visceral artery aneurysms are rare, with an average incidence of approximately 0.1% to 2% (Hossain et al, 2001; Panayiotopoulos et al, 1996). Splenic artery aneurysms account for approximately 60% of all visceral aneurysms, followed by hepatic artery aneurysms, which constitute 20% (Abbas et al, 2003). Hepatic artery aneurysms were initially described by Wilson in 1809 (O’Connor et al, 1995). The first successful surgical repair was performed by Kehr in 1903, in which he ligated the feeding vessel proximal to the hepatic artery (Carr et al, 1996; Guida & Moore, 1966). Within the past 2 decades, endovascular therapy has been utilized with increasing frequency, and O’Connor and colleagues reported successful endovascular stent exclusion of a hepatic artery aneurysm in 1995.
Hepatic artery aneurysms are more common in men, with a 2 : 1 prevalence (Abbas et al, 2003; Panayiotopoulos et al, 1996). The mean age of presentation is generally around 60 years of age, but hepatic artery aneurysms have been reported in all age groups (Abbas et al, 2003). The etiology of nontraumatic hepatic artery aneurysms remains unclear. True aneurysms undergo dilation and thinning of the vessel wall, although the blood is still contained within the vessel wall (Ikeda et al, 2008). A common histopathologic feature is medial degeneration of the arterial wall, which may be congenital but is further stressed by various factors (Abbas et al, 2003; Panayiotopoulos et al, 1996). Atherosclerosis is present in approximately 30% of aneurysms, but it is debatable whether it is a causative event or a secondary phenomenon (Messina & Shanley, 1997).
Several other conditions have been associated with hepatic artery aneurysms; these include arterial fibrodysplasia, vasculitis, polyarteritis nodosa, systemic lupus erythematous, tuberculosis, Marfan syndrome, Ehler-Danlos syndrome, arteritis, and hyperflow conditions (Abbas et al, 2003; Ikeda et al, 2008; Panayiotopoulos et al, 1996; Messina & Shanley, 1997). In the early twentieth century, most true hepatic artery aneurysms were mycotic, with bacterial endocarditis being the most common cause. With the advent of antibiotics, this form is generally only found in intravenous drug users (Shanley et al, 1996a).
Approximately 50% of all hepatic artery aneurysms are false aneurysms, or pseudoaneurysms, caused by a ruptured arterial wall with subsequent periarterial hematoma formation. These are generally the result of trauma, iatrogenic injury, inflammation, or infection (Carr et al, 1996; Guida & Moore, 1966). Pseudoaneurysms that result from iatrogenic injury to the hepatic arterial system are usually secondary to biliary, hepatic, or pancreatic interventions and to the laparoscopic or open treatment of abdominal and retroperitoneal pathologies (Bulut et al, 2002; Duce et al, 2002; Grego et al, 2003; Ikeda et al, 2008; Larson et al, 2002; Tessier et al, 2003; Tulsyan et al, 2007; see Chapters 28, 33, 34, and 54). Aneurysms resulting from laparoscopic cholecystectomy frequently affect the right hepatic artery but may be confined to the cystic artery remnant (Tessier et al, 2003). Pancreatitis and other inflammatory diseases can damage the arterial wall and lead to pseudoaneurysm formation (Mallick & Winslet, 2004). Additionally, hepatic artery pseudoaneurysm after resection of a hilar cholangiocarcinoma has been reported (Briceno et al, 2008).
Most hepatic artery aneurysms are solitary (80%), either saccular or fusiform, with a maximum diameter ranging from 1 to 14.5 cm (Abbas et al, 2003; Shanley et al, 1996). Other concomitant visceral artery aneurysms are present 31% of the time, and nonvisceral artery aneurysms are evident in 42% (Abbas et al, 2003). The majority, 66% to 80%, occur extrahepatically; however, the incidence of intrahepatic aneurysms may be increasing, compared with extrahepatic aneurysms (Abbas et al, 2003; Messina & Shanley, 1997). This change in presentation is likely the result of increasing use of percutaneous and laparoscopic interventions and also of improved imaging modalities utilized in the trauma setting (Kasirajan et al, 2001).
In one review of reported cases from 1985 to 1995, the right hepatic artery was found to be most commonly affected (47%), followed by the common hepatic artery (22%), the proper hepatic artery (16%), the left hepatic artery (13%), and rarely the cystic artery (1%) (Shanley et al, 1996). The natural history of these lesions is that of progressive growth, and it is probable that increasing size is accompanied by an increasing rate of rupture, in spite of a paucity of supporting evidence (Abbas et al, 2003). Nonatherosclerotic aneurysms carry a higher risk of rupture than atherosclerotic aneurysms (Abbas et al, 2003).
The lifetime risk of rupture for hepatic artery aneurysm ranges from 14% to 80% (Abbas et al, 2003; Carr et al, 2001; Dolapci et al, 2003; Ikeda et al, 2008; Lagana et al, 2006; Panayiotopoulos et al, 1996), and the mortality rate for ruptured hepatic artery aneurysms is 3% to 40% (Abbas et al, 2003; Ikeda et al, 2008; Panayiotopoulos et al, 1996; Shanley et al, 1996; Tessier et al, 2003). Rupture can occur into the peritoneal cavity (43%), biliary tree (41%), gastrointestinal (GI) tract (11%), or portal vein (5%) (Carr et al, 2001). Abdominal pain is often present, usually in the epigastrium with radiation to the back or right shoulder. Approximately 60% of patients with rupture come to medical attention in hypovolemic shock.
In 1871, Quincke described jaundice, hemobilia (see Chapter 105), and biliary colic in a patient with a hepatic artery aneurysm. These symptoms have become known as the classic triad, but in actuality, they are present in fewer than 40% of cases (Messina & Shanley, 1997). These symptoms are caused by erosion into the biliary tree, which causes intraductal clot or external compression of the bile duct (Messina & Shanley, 1997); rupture into the bile duct causes hemobilia. Occasionally, with a large hepatic artery aneurysm, a mass may be palpated in the upper abdomen, often with an associated bruit or thrill; however, pulsatile masses and bruits are uncommon in intact aneurysms. Expanding aneurysms can cause upper abdominal discomfort with pain radiating into the back, and pseudoaneurysms that result from placement of transhepatic biliary drainage catheters often manifest with a sentinel hemorrhage and blood in the collection bag.
With recent advances in cross-sectional imaging and arteriography, true hepatic artery aneurysms are being detected earlier in their course. Asymptomatic aneurysms (30% to 60%) may be discovered incidentally during radiologic investigation performed for other indications (O’Connor et al, 1995; Panayiotopoulos et al, 1996; Tulsyan et al, 2007). On plain radiographs, a hepatic artery aneurysm may appear as an eggshell-like calcification in the right upper quadrant (O’Driscoll et al, 1999). If this diagnosis is suspected, further investigation with contrast-enhanced computed tomography (CT) scan or magnetic resonance angiography is warranted to delineate the extent of the lesion and define its relationship to surrounding structures. Angiography (see Chapter 19) can be used to characterize hepatic artery blood flow prior to operative treatment (Messina & Shanley, 1997), but ultrasound is rarely used to diagnose hepatic artery aneurysms. A hepatic artery aneurysm may be discovered during abdominal surgery for another indication and will appear as a calcified nodule on the hepatoduodenal ligament.
Improvements in the quality and availability of cross-sectional imaging (see Chapters 16 and 17) have led to an increasing number of aneurysms being detected prior to rupture. Although it is unclear whether the actual incidence of true hepatic artery aneurysms is increasing, incidental discovery during imaging performed for unrelated reasons has increased. For example, the routine use of CT scan in trauma patients has led to increased detection of false aneurysms of the intrahepatic arterial branches (Messina & Shanley, 1997). Also, the increased use of diagnostic and therapeutic biliary interventions have contributed to the increasing incidence of false aneurysms (Messina & Shanley, 1997).
Recent studies demonstrate that a selective approach can be used to manage asymptomatic hepatic artery aneurysms. Currently, no consensus exists regarding size criteria for intervention, but many advocate that small (<2 cm) lesions can be safely observed (Abbas et al, 2003; Ikeda et al, 2008); however, surgical repair, ligation, or embolization should be considered for aneurysms larger than 2 cm in a patient who is a reasonable operative risk with a life expectancy greater than 2 years. In patients with marginal or poor health and aneurysms that measure 2 to 5 cm, careful observation may be warranted (Abbas et al, 2003). The presence of multiple aneurysms is a risk factor for rupture and warrants intervention. Likewise, it is generally recommended that all pseudoaneurysms should be treated, given the high risk of rupture that they pose.
Although some centers allow for a degree of permissive hypotension, the management of ruptured hepatic artery aneurysms consists of volume resuscitation and correction of coagulopathy followed by definitive treatment involving surgical repair, embolization, occlusion, or endovascular stenting (Carr et al, 2001). Occasionally, angiographic intervention may be used as an adjunct prior to repair. In the elective setting, the choice of open surgical repair versus endovascular treatment depends on many factors, including the size and anatomy of the aneurysm, the shape of the sac and its accessibility to endovascular device placement or embolization, the need to restore arterial continuity, and the general health of the patient. A past failure of endovascular intervention does not necessarily preclude further attempts.
Open repair of hepatic artery aneurysms depends on the anatomy and location of the aneurysm, collateral blood flow, operative risk, and clinical status. In the elective setting, the anatomy of the aneurysm, delineation of arterial circulation, and identification of collateral vessels in the port hepatic are ideally determined preoperatively by angiography. In general, aneurysms of the common hepatic artery may be ligated, with or without resection of the aneurysm sac, as long as the portal vein is patent. Reconstruction is usually unnecessary secondary to collateral circulation via the gastroduodenal and right gastric arteries. Failure to confirm adequate collateral vessel circulation can lead to hepatic necrosis (Rokke et al, 1997).
If the patient has underlying hepatic parenchymal disease or is in a state of hemorrhagic shock, reconstruction is recommended, because the liver will be more sensitive to ischemia (Messina & Shanley, 1997; Shanley et al, 1996). Arterial reconstruction is recommended for aneurysms of the proper hepatic artery and its extrahepatic branches, because ligation may interfere with collateral circulation and may induce ischemic necrosis. Autogenous vein grafts, synthetic grafts, aneurysmorraphy with vein patch closure, and aortohepatic bypass have been utilized to restore blood flow. Aortohepatic bypass with saphenous vein or polytetrafluoroethylene (PTFE) graft that originates at the supraceliac aorta is generally preferred when bypass is required.
Intrahepatic aneurysms usually require ligation of the branch hepatic arteries and may require liver resection. Simple ligation of proximal vessels can help control bleeding intrahepatic aneurysms and may be a safer alternative to resection in critically ill patients, despite the risk of necrosis. In all hepatic aneurysms, vascular control can be gained from within the aneurysm, if surrounding inflammation prevents adequate exposure and dissection of adjacent arteries (Messina & Shanley, 1997). Complications after surgical repair are generally related to ischemic necrosis of the liver, abscess formation, and sepsis (Abbas et al, 2003).
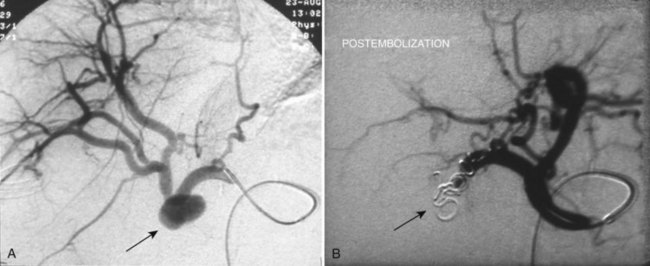
Endovascular management of hepatic artery aneurysms has become increasingly popular over the past decade and is particularly useful for treating pseudoaneurysms that arise from iatrogenic injuries (Figs. 104.1 and 104.2). These procedures offer an alternative to conventional open surgical intervention with the benefit of lower morbidity and mortality (Ikeda et al, 2008; Larson et al, 2002; Saltzberg et al, 2005; Tulsyan et al, 2007). Recent studies found rates of technical success from 75% to 98% (Kasirajan et al, 2001; Mallick & Winslet, 2004; Sachdev et al, 2006).
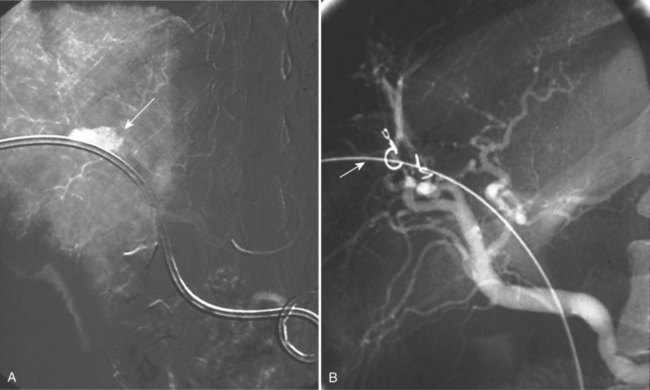
FIGURE 104.1 Hepatic pseudoaneurysm. A, After percutaneous biliary stent insertion (arrow). B, Managed by embolization (arrow).
Various minimally invasive techniques are available to treat aneurysms and pseudoaneurysms. Selective catheterization of the involved vessel and embolization with coils or polymerizing agents has been used for ablation of hepatic artery aneurysms, and percutaneous embolization is being used with increasing frequency in cases of emergent aneurysm rupture (Tulsyan et al, 2007). Endovascular stent grafts allow for preservation of end-organ flow and exclusion of the aneurysm. The arterial anatomy and the location of the aneurysm have a significant impact on the technical ability to place a stent graft (Larson et al, 2002); sufficient normal caliber artery must be available on either side of the aneurysm to allow for a proper stent graft seal and aneurysm exclusion, although further studies are needed to elucidate the long-term durability of stents.
The tortuosity and redundancy of the visceral vessels can increase the difficulty of endovascular interventions. Migration of embolic material and stent graft occlusion are recognized complications of transcatheter treatment. Additional complications include endoleak, failure to completely occlude the aneurysm, hepatic ischemia, and recanalization (Abbas et al, 2003; Kasirajan et al, 2001).
Hepatic Arteriovenous Fistulae and Shunts
Congenital Hepatic Vascular Shunts
The paired umbilical veins bring oxygenated blood to the embryo and course on either side of the liver. When they contact the hepatic sinusoids, the right umbilical vein and portions of the left umbilical vein become obliterated; the persistent left umbilical vein carries blood from the placenta to the fetus. A large channel, the ductus venosus, connects the left umbilical vein to the inferior vena cava to allow oxygenated blood to bypass sinusoid circulation (Gallego et al, 2004). Any deviation from the normal vascular system’s embryologic development can lead to abnormal fistulae and shunting (Fig. 104.3).
Related posts:
 Preoperative and postoperative nutrition in hepatobiliary surgery
Preoperative and postoperative nutrition in hepatobiliary surgery
 Portal hypertension in children
Portal hypertension in children
 Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
Chemotherapy and radiotherapy for pancreatic and periampullary cancer: Adjuvant, neoadjuvant, and palliative
 Distal splenorenal shunt
Distal splenorenal shunt
 Magnetic resonance imaging of the liver, biliary tract, and pancreas
Magnetic resonance imaging of the liver, biliary tract, and pancreas
 Interventional endoscopy: Technical aspects
Interventional endoscopy: Technical aspects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


