Fig. 5.1
An approximate 2–2.5-cm longitudinal incision is made from the center of the umbilicus (a). The fascial defect (b) is grasped with Kocher forceps (c)
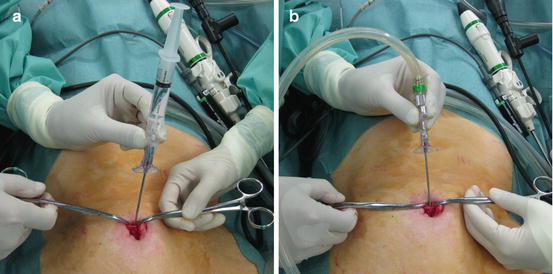
Fig. 5.2
An insufflation needle is inserted (a) for creation of pneumoperitoneum after a saline test (b)
After creation of pneumoperitoneum, a 5-mm trocar suitable for optical viewing (Versaport Bladeless Optical Trocar or Xcel Trocar (Ethicon Johnson & Johnson, Cincinnati, OH, US), with a forward viewing scope (5 mm in diameter) is inserted via the fascial defect. If no 0-degree rigid scope is available, a 30-degree rigid scope can also be used. While the operator twists the trocar, an assistant holds the laparoscope to prevent excess insertion force due to its weight (Fig. 5.3). After assuring that the trocar is in the free abdominal cavity, the obturator is pulled out, and a Karl Storz Hopkins telescope (30°, 5.5 mm in diameter, 50 cm in length) is used with a high definition camera system. Because the scope is 50 cm in length, interference between the scope head and the forceps handles is prevented. During the operation, if a linear stapler is required, the 5-mm camera trocar is replaced with a 12-mm trocar (Fig. 5.4a–d). When forceps larger than 5 mm in diameter is needed, the same methodology is applied. However, for this procedure, opening the incision with Kelly clamp or an additional skin incision is often required. Fascial incision is not usually required, and an unnecessary incision can lead to gas leakage.

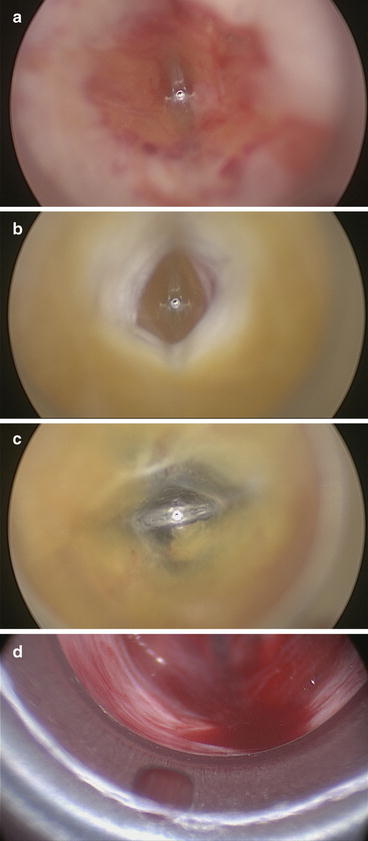
Fig. 5.3
While the operator twists the optical trocar, the assistant stands to the patient’s right and holds the laparoscope to prevent excess insertion force due to its weight
Fig. 5.4
View of the optical method: (a) edge of the fascial defect (fascia), (b) the fascia (white layer), and (c) fat (yellow layer); (d) 30-degree scope penetrates the peritoneum (white) and reaches the abdominal cavity
Two trocars are then inserted. We normally use trocars of different lengths with a relatively small head, such as EndoTIP cannulas (both 6 mm in diameter), one 6 cm long and the other 10.5 cm long. These trocars are reusable and are thus economical. First an isosceles triangle centered on the line between the target organ as the vertex and the camera trocar insertion point is assumed, and the ports are inserted at the both ends of the incision corresponding to the angles at the base of the triangle. It is then possible to set the ports coaxially and to maximize the distance between them. Ports are inserted with a twisting motion, without any additional fascial incision. By using ports of different lengths, the port heads will be prevented from hitting each other. When the ports are inserted, the scope is replaced with a 50-cm 30-degree scope (Karl Storz-Endoskope, Tuttlingen, Germany). Use of a high definition system provides high quality viewing of the operation even though the scope is as small as 5 mm in diameter. The secret to success with this method is the best possible vertical insertion of both the camera trocar and the EndoTIP cannulas. When the devices are inserted obliquely, the procedure takes time because they slide along the abdominal wall. In addition, vertical insertion increases the safety of the procedure because insertion of the EndoTIP cannulas can be monitored through the transparent side wall of the camera trocar. Because all of the devices can be inserted without any additional fascial incision, this method minimizes injury at the insertion site. In addition, because the devices can be tightly inserted, there is no need for concern over leakage of the pneumoperitoneum gas (Fig. 5.5a–d).
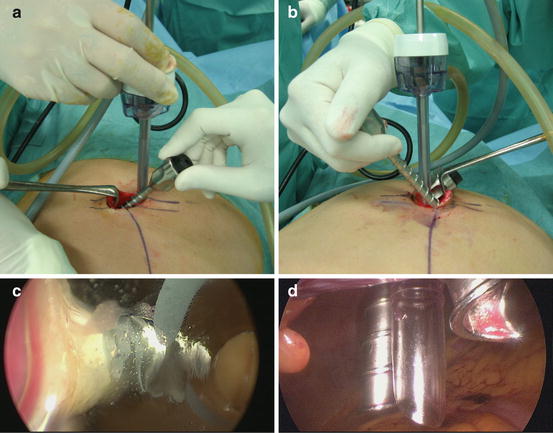
Fig. 5.5




(a, b) Endo TIP cannulas, 6.5 and 10.5 cm in length, are screwed in on both sides of the incision; (c) insertion of the EndoTIP cannulas is monitored through the transparent side wall of the camera trocar; (d) view of the umbilical site after trocar insertion
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
