Abdominal Rectopexy: Hand-Assisted
Edward Borrazzo
Neil Hyman
Rectal prolapse may cause considerable life-altering disability including bleeding, pain, and fecal incontinence. Numerous remedial operations have been described with very few high quality studies available to facilitate evidence-based recommendations (1).
Generally speaking, abdominal approaches are recommended for fit patients and perineal procedures for the elderly and infirmed. Rectopexy allows for fixation of the rectum to the sacrum, thereby preventing the rectum from prolapsing out the anal canal. The role/need for concomitant resection remains uncertain and controversial (2,3).
Rectopexy can be performed utilizing open, laparoscopic, or hybrid techniques, such as the hand-assisted laparoscopic approach. It is our custom to perform rectopexies (with or without resection) using a purely laparoscopic approach. However, patients with recurrent prolapse after a previous abdominal approach (either open or laparoscopic) are often best-served by hand-assisted laparoscopic technique. Similarly, a hand-assisted laparoscopic rectopexy can be used to obviate the need for conversion to full open surgery when technical problems are encountered during laparoscopic rectopexy.
Extensive adhesions or previous pelvic sepsis can be considered a relative contraindication to hand-assisted laparoscopic rectopexy; however it is often difficult to predict a hostile pelvis based on history alone. Laparoscopic visualization with a forthright, considered assessment of the local conditions is often an appropriate first step.
As in all operative procedures, the surgeon must candidly assess their skill set and decide what is safest for the patient in their hands. Hand-assisted laparoscopic rectopexy may be the best and safest approach for many surgeons. The patient is primarily owed a safe and effective procedure to correct their prolapse and minimize the risk or recurrence. Whether the procedure is performed open, laparoscopically, or with hand assistance is truly a secondary consideration.
Planning is similar to any other abdominal colorectal procedure. Patients should be suitable for laparotomy/laparoscopy or a perineal procedure should be chosen. It is important to consider why the patient has developed the prolapse and whether there are other manifestations of pelvic floor relaxation.
A careful history may elicit causative factors for the prolapse such as bulimia or a connective tissue disorder. Patients who strain excessively and/or have a defecation disorder such as a non-relaxing puborectalis can be appropriately counseled or referred for biofeedback to minimize the risk of recurrence after corrective surgery. Those individuals suspected to have slow-transit constipation may be scheduled for colonic transit studies and considered for colectomy at the time of rectopexy on a highly selective basis. Women with concomitant uterine prolapse or cystocele, for example, can be treated in a multidisciplinary manner with a joint surgical approach.
Flexible endoscopy (or suitable radiologic studies) should usually be performed, especially in age-appropriate patients, to make sure that the rectal prolapse is not caused by a neoplasm that is acting as the lead point for the prolapse.
If the patient has recurrent prolapse and/or has undergone previous pelvic surgery, review of the previous operative report(s) can be invaluable. Quite often, “recurrent” prolapse actually is persistent prolapse and represents a failure to adequately mobilize the rectum by an inexperienced pelvic surgeon.
Hand-assisted laparoscopic techniques are helpful for dissection of the mid and lower rectum, especially in reoperative cases. An intracorporeal hand can facilitate identification of the ureters if stents are used, and also provides countertraction for dissection of the lower third of the rectum down to the pelvic floor. Tactile sensation affords better assessment of the true tension on the rectum and the appropriate degree of superior traction when fixing the rectum to the sacral promontory.
We position the hand-assisted device at the level of the umbilicus (Fig. 53.1). This keeps the hand from obscuring the field of view as compared to more inferior placement and provides acceptable cosmesis with the subsequent incision hidden in the umbilical fold. Ports are placed in the mid-abdomen on each side. An additional working port is placed in the right lower quadrant. The camera alternates between the two lateral ports to get a view on each side of the rectum as the dissection is performed in the pelvis.
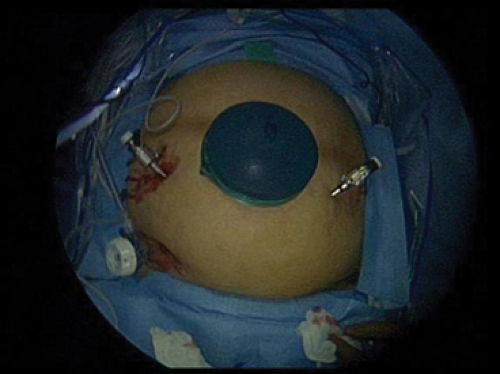 Figure 53.1 Port position. Operating surgeon stands on the patient’s right side. The handport is positioned at the umbilicus. The two mid abdominal ports, here 5 mm, are used for the laparoscope and assistant retractor, alternating sides as needed. Right hand working port is in the right lower quadrant. |
In reoperative cases, anatomic planes are often difficult to identify visually at first. Use of the hand can help define the proper plane of dissection. It is often easiest to get




Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
