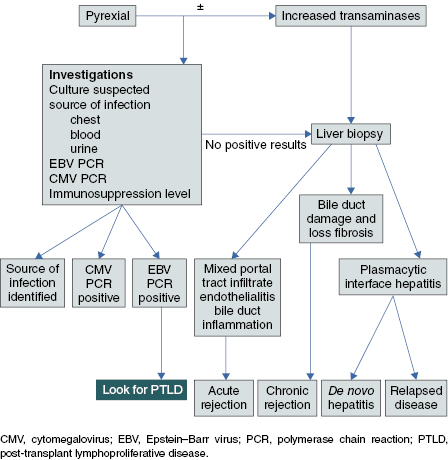
Algorithm 32.1 Investigations post liver transplant
Management
- Rejection:
- Acute: pulsed methyl prednisolone 10 mg/kg/day IV for 3 days with ranitidine. Maintenance immunosuppression should be increased or other agents added [mycophenolate mofitil (MMF) (10–20 mg/kg twice daily)]
- Chronic: Increase immunosuppression, add other drugs (e.g. MMF, sirolimus). Ursodeoxycholic acid (10 mg/kg twice daily) if bile duct damage/obstruction. Re-transplantation may be required
- Acute: pulsed methyl prednisolone 10 mg/kg/day IV for 3 days with ranitidine. Maintenance immunosuppression should be increased or other agents added [mycophenolate mofitil (MMF) (10–20 mg/kg twice daily)]
- Infection:
- CMV: ganciclovir IV (5 mg/kg twice daily) for 3 weeks
- EBV: there is no specific treatment for EBV. Immunosuppression should be reduced. The identification of EBV should prompt investigation of PTLD
- Any infection may present due to immunosuppression
- CMV: ganciclovir IV (5 mg/kg twice daily) for 3 weeks
- Relapse of autoimmune disease: increase in immunosuppression with steroids, MMF or azathioprine. Re-transplant may be necessary if severe
- De novo
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



