10 Urethral Diverticulectomy
 Videos
VideosTo view the videos discussed in this chapter, please go to expertconsult.com. To access your account, look for your activation instructions on the inside front cover of this book.
In many cases the diagnosis of urethral diverticulum is made (or suspected) on physical examination. The presence of a suburethral mass, often tender, with expression of discharge by urethra when the anterior vaginal wall is massaged is a typical finding. The differential diagnosis includes cystocele, anterior vaginal wall cyst, adenoma, and ectopic ureter. In these cases there is no expression of urethral discharge on palpation. The diagnosis can be confirmed by a number of imaging tests, including voiding cystourethrography (VCUG), ultrasonography, and magnetic resonance imaging (MRI). We prefer to obtain an MRI scan in all cases of known or suspected urethral diverticulum because it precisely defines the anatomy (size, location, shape, and number of diverticula) and aids in surgical dissection and removal (Figs. 10-1 through 10-3). A diverticular ostium is seen on urethroscopy in most, but not all, cases. Although urethroscopy can identify the location of the urethral communication, it tells nothing about the size, location, and anatomy of the diverticulum itself. Also, in cases of urethral pain, urethroscopy can be painful and at times even impossible with only local anesthesia. In those cases we reserve urethroscopy for the operating room at the time of surgical excision.
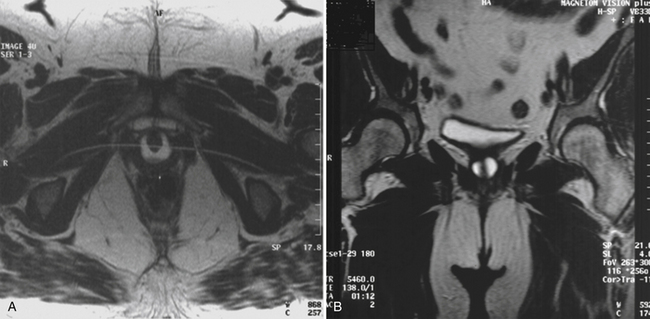
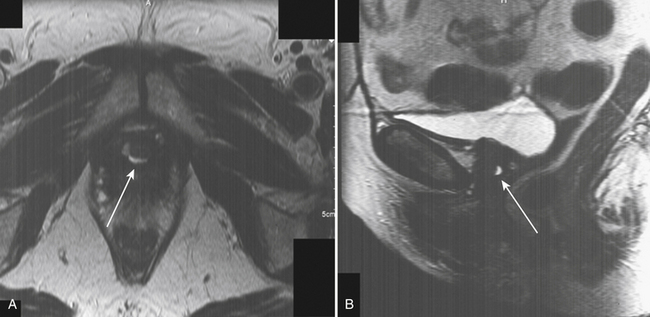
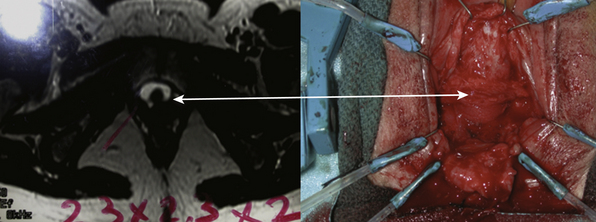
Figure 10-3 Axial magnetic resonance image (left) reveals a large circular diverticulum that is deficient ventrally. This information was invaluable at surgery, when a fibrous band of tissue was found and the diverticulum was identified laterally on both sides (right). (See Case #3.)
Ancillary testing can be performed in certain circumstances. For example, when stress incontinence is suspected, urodynamic testing can confirm the diagnosis. This could lead the surgeon to decide to perform an antiincontinence procedure at the same time the diverticulum is repaired.
Surgical Repair of Urethral Diverticulum
1. Create well-vascularized flaps.
2. Know and identify all appropriate anatomical layers and structures.
3. Identify normal urethra before excising the diverticulum.
4. Excise the entire diverticulum (preferable) or the entire mucosal portion along with the communication to the urethra.
5. Avoid excision of normal urethra.
6. Ensure a watertight reconstruction of the urethra.
7. Perform multilayered, nonoverlapping closure of the urethra.
Surgical Technique for Urethral Diverticulectomy
1. Create a well-vascularized vaginal flap. We prefer an inverted-U incision, because it creates excellent exposure and allows for nonoverlapping suture lines at closure (Fig. 10-4
Related posts:
 Pelvic Organ Prolapse: Introduction, Nonsurgical Management, and Planning of Surgical Repair
Pelvic Organ Prolapse: Introduction, Nonsurgical Management, and Planning of Surgical Repair
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


